

A New Vision for Therapeutic Hypothermia in the Era of Targeted Temperature Management: A Speculative Synthesis
- PMID: 30802174
- PMCID: PMC6434603
- DOI: 10.1089/ther.2019.0001
A New Vision for Therapeutic Hypothermia in the Era of Targeted Temperature Management: A Speculative Synthesis
Abstract
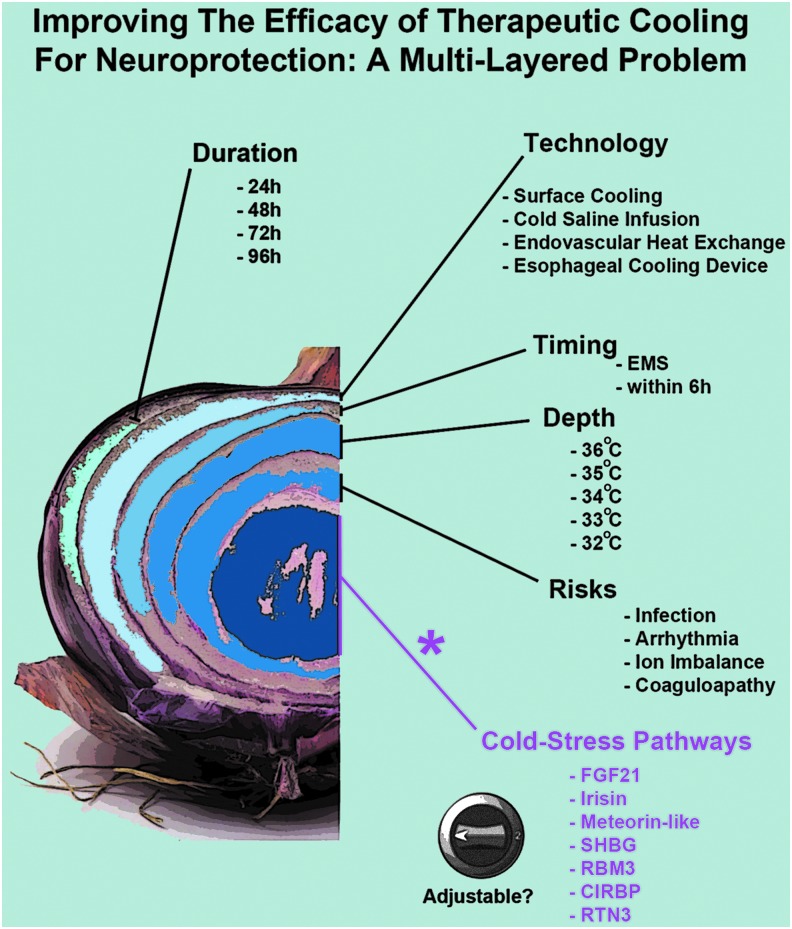
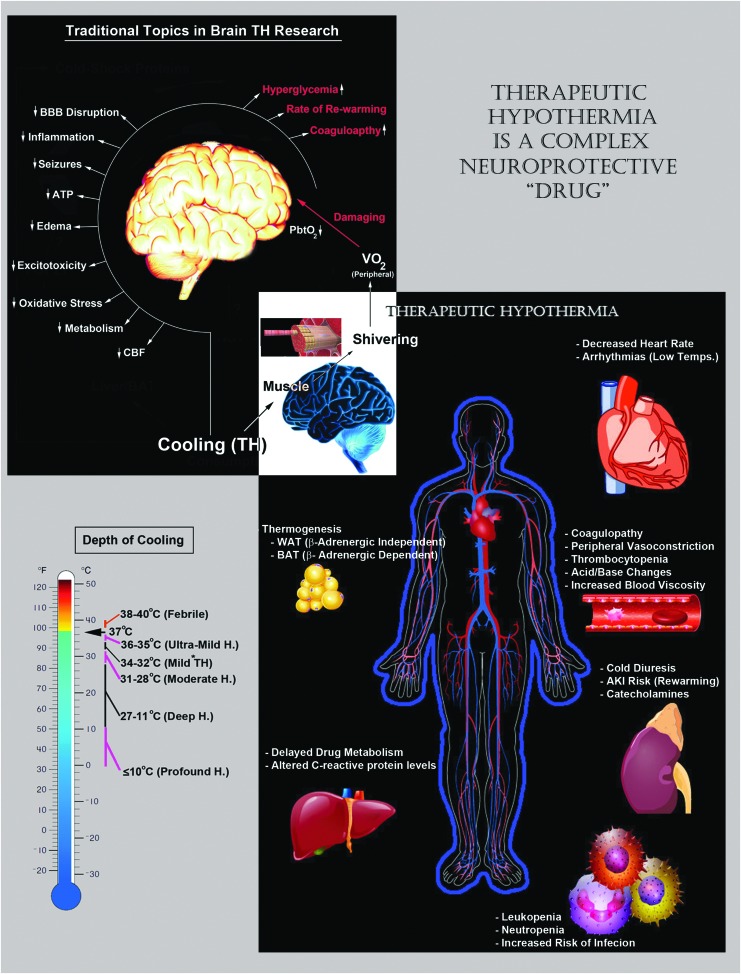
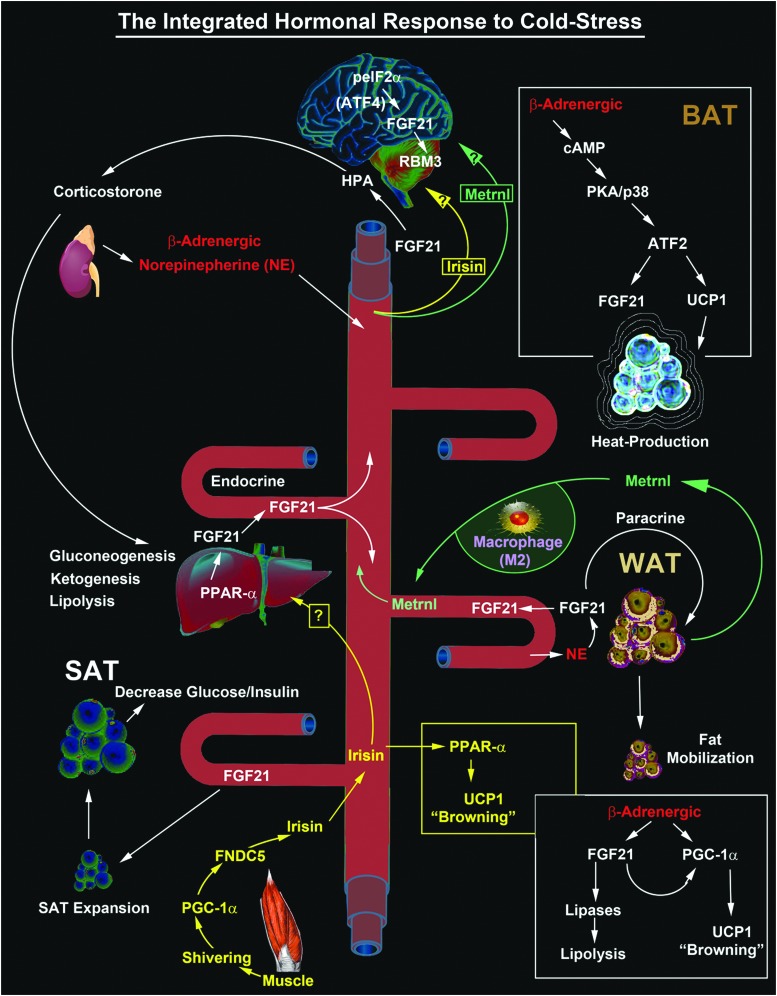
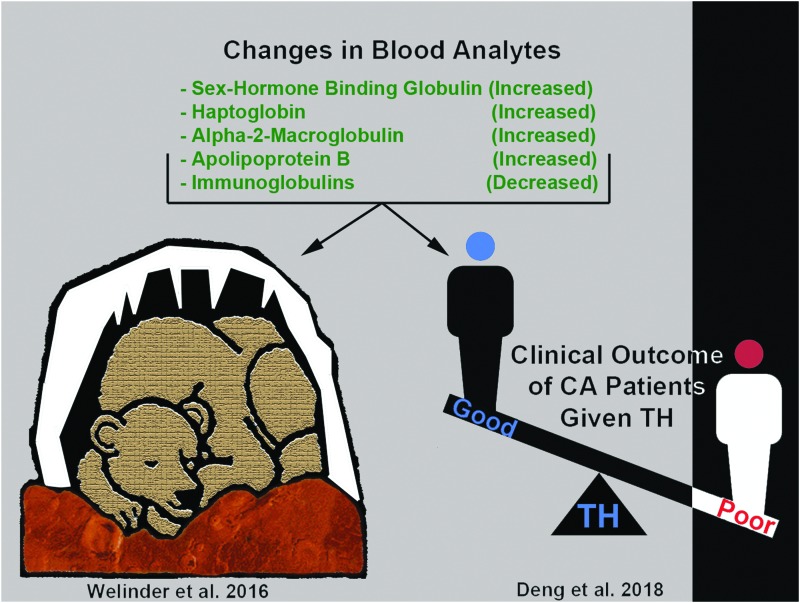
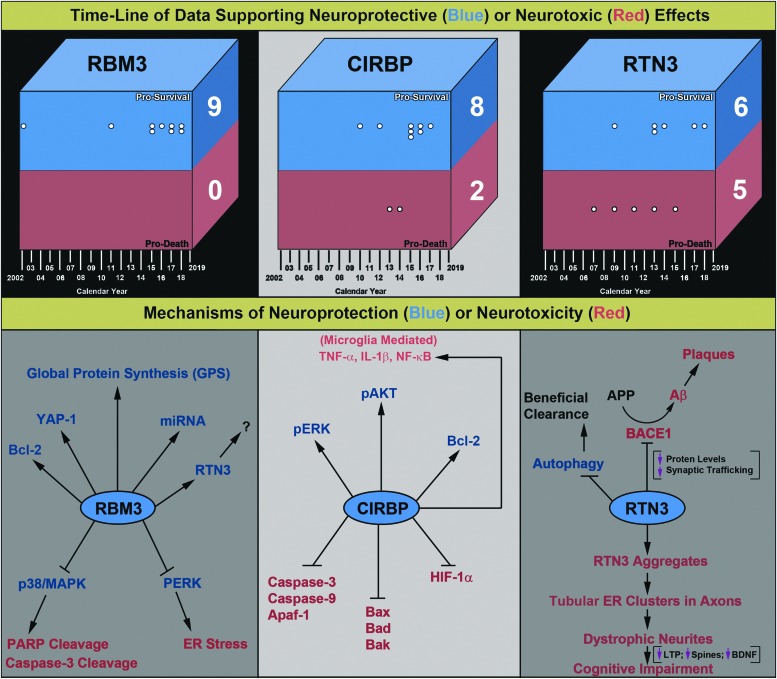
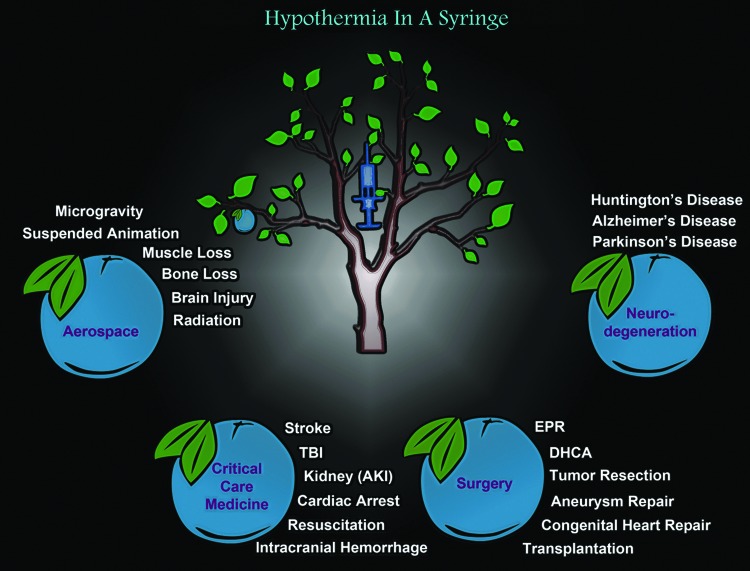
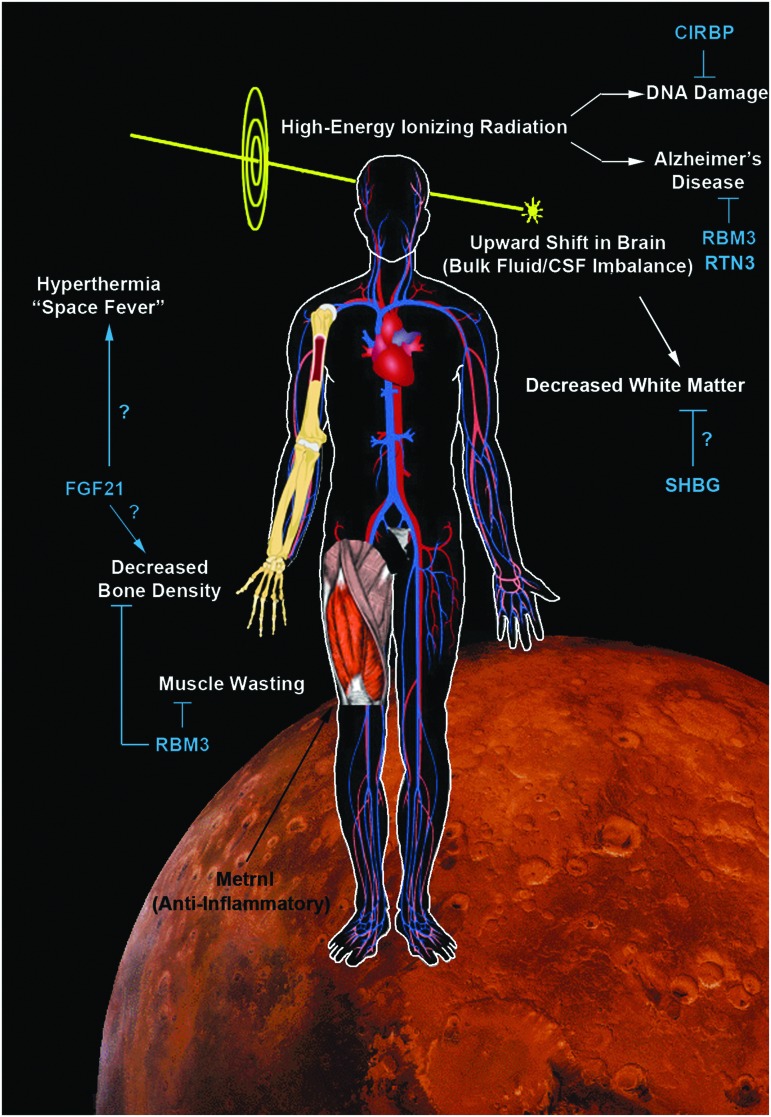
Three decades of animal studies have reproducibly shown that hypothermia is profoundly cerebroprotective during or after a central nervous system (CNS) insult. The success of hypothermia in preclinical acute brain injury has not only fostered continued interest in research on the classic secondary injury mechanisms that are prevented or blunted by hypothermia but has also sparked a surge of new interest in elucidating beneficial signaling molecules that are increased by cooling. Ironically, while research into cold-induced neuroprotection is enjoying newfound interest in chronic neurodegenerative disease, conversely, the scope of the utility of therapeutic hypothermia (TH) across the field of acute brain injury is somewhat controversial and remains to be fully defined. This has led to the era of Targeted Temperature Management, which emphasizes a wider range of temperatures (33-36°C) showing benefit in acute brain injury. In this comprehensive review, we focus on our current understandings of the novel neuroprotective mechanisms activated by TH, and discuss the critical importance of developmental age germane to its clinical efficacy. We review emerging data on four cold stress hormones and three cold shock proteins that have generated new interest in hypothermia in the field of CNS injury, to create a framework for new frontiers in TH research. We make the case that further elucidation of novel cold responsive pathways might lead to major breakthroughs in the treatment of acute brain injury, chronic neurological diseases, and have broad potential implications for medicines of the distant future, including scenarios such as the prevention of adverse effects of long-duration spaceflight, among others. Finally, we introduce several new phrases that readily summarize the essence of the major concepts outlined by this review-namely, Ultramild Hypothermia, the "Responsivity of Cold Stress Pathways," and "Hypothermia in a Syringe."
Keywords: FGF21; RBM3; hypoxic/ischemic encephalopathy; space; targeted temperature management; therapeutic hypothermia.
Conflict of interest statement
T.C.J and P.M.K. are coinventors on a pending patent on the use of FGF21 therapy in temperature-managed patients titled: “Method to Improve Neurologic Outcomes in Temperature Managed Patients” (USPTO application No. 15/573,006). P.M.K. is also a copatent holder on an invention for the use of rapid induction of deep hypothermia after cardiopulmonary arrest titled “Method of Inducing EPR Following Cardiopulmonary Arrest” (US 8,628,512 B2).
Figures
Similar articles
-
Cold protection allows local cryotherapy in a clinical-relevant model of traumatic optic neuropathy.Elife. 2022 Mar 30;11:e75070. doi: 10.7554/eLife.75070. Elife. 2022. PMID: 35352678 Free PMC article.
-
[Therapeutic hypothermia for severe traumatic brain injury].Ann Fr Anesth Reanim. 2013 Nov;32(11):787-91. doi: 10.1016/j.annfar.2013.09.004. Epub 2013 Oct 15. Ann Fr Anesth Reanim. 2013. PMID: 24138767 Review. French.
-
Therapeutic hypothermia and targeted temperature management in traumatic brain injury: Clinical challenges for successful translation.Brain Res. 2016 Jun 1;1640(Pt A):94-103. doi: 10.1016/j.brainres.2015.12.034. Epub 2015 Dec 30. Brain Res. 2016. PMID: 26746342 Free PMC article. Review.
-
Is there still a role for hypothermia in neurocritical care?Curr Opin Crit Care. 2017 Apr;23(2):115-121. doi: 10.1097/MCC.0000000000000398. Curr Opin Crit Care. 2017. PMID: 28234783 Review.
-
Emerging Trends in the Use of Therapeutic Hypothermia as a Method for Neuroprotection in Brain Damage (Review).Sovrem Tekhnologii Med. 2021;12(5):94-104. doi: 10.17691/stm2020.12.5.11. Epub 2020 Oct 28. Sovrem Tekhnologii Med. 2021. PMID: 34796010 Free PMC article. Review.
Cited by
-
Identification of Metabolomic Signatures for Ischemic Hypoxic Encephalopathy Using a Neonatal Rat Model.Children (Basel). 2023 Oct 16;10(10):1693. doi: 10.3390/children10101693. Children (Basel). 2023. PMID: 37892356 Free PMC article.
-
Hypoxia-ischemia-mediated effects on neurodevelopmentally regulated cold-shock proteins in neonatal mice under strict temperature control.Pediatr Res. 2022 Feb 19:10.1038/s41390-022-01990-4. doi: 10.1038/s41390-022-01990-4. Online ahead of print. Pediatr Res. 2022. PMID: 35184138 Free PMC article.
-
Cerebral Edema in Traumatic Brain Injury: a Historical Framework for Current Therapy.Curr Treat Options Neurol. 2020 Mar;22(3):9. doi: 10.1007/s11940-020-0614-x. Epub 2020 Mar 3. Curr Treat Options Neurol. 2020. PMID: 34177248 Free PMC article.
-
Hypothermia reduces glymphatic transportation in traumatic edematous brain assessed by intrathecal dynamic contrast-enhanced MRI.Front Neurol. 2022 Oct 20;13:957055. doi: 10.3389/fneur.2022.957055. eCollection 2022. Front Neurol. 2022. PMID: 36341130 Free PMC article.
-
Associations between RNA-Binding Motif Protein 3, Fibroblast Growth Factor 21, and Clinical Outcome in Patients with Stroke.J Clin Med. 2022 Feb 11;11(4):949. doi: 10.3390/jcm11040949. J Clin Med. 2022. PMID: 35207221 Free PMC article.
References
-
- Adelson PD, Wisniewski SR, Beca J, Brown SD, Bell M, Muizelaar JP, Okada P, Beers SR, Balasubramani GK, Hirtz D; Paediatric Traumatic Brain Injury Consortium. Comparison of hypothermia and normothermia after severe traumatic brain injury in children (Cool Kids): a phase 3, randomised controlled trial. Lancet Neurol 2013;12:546–553 - PubMed
-
- Alonso-Alconada D, Broad KD, Bainbridge A, Chandrasekaran M, Faulkner SD, Kerenyi A, Hassell J, Rocha-Ferreira E, Hristova M, Fleiss B, Bennett K, Kelen D, Cady E, Gressens P, Golay X, Robertson NJ. Brain cell death is reduced with cooling by 3.5 degrees C to 5 degrees C but increased with cooling by 8.5 degrees C in a piglet asphyxia model. Stroke 2015;46:275–278 - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical