

Increasing contribution of integrated forms to total HIV DNA in blood during HIV disease progression from primary infection
- PMID: 30803934
- PMCID: PMC6442355
- DOI: 10.1016/j.ebiom.2019.02.016
Increasing contribution of integrated forms to total HIV DNA in blood during HIV disease progression from primary infection
Abstract
Background: In the current context of research on HIV reservoirs, offering new insights into the persistence of HIV DNA in infected cells, which prevents viral eradication, may aid in identifying cure strategies. This study aimed to describe the establishment of stable integrated forms among total HIV DNA during primary infection (PHI) and their dynamics during the natural history of infection.
Methods: Total and integrated HIV DNA were quantified in blood from 74 PHI patients and 97 recent seroconverters (<12 months following infection, "progression cohort"). The evolution of both markers over six years was modelled (mixed-effect linear models). Their predictive values for disease progression were studied (Cox models).
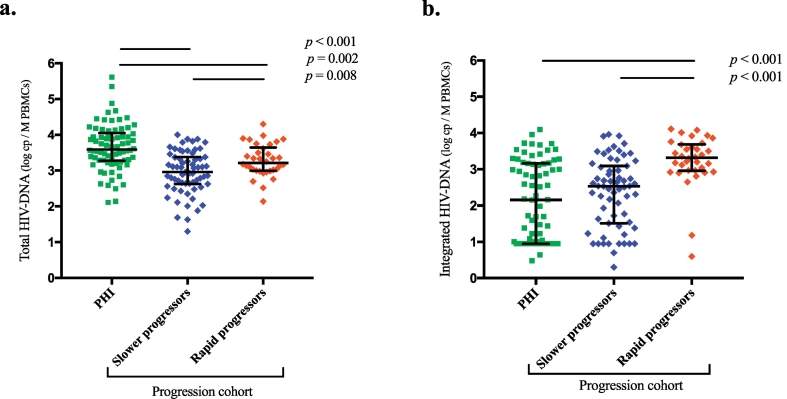
Findings: For most patients during PHI, stable integrated forms were a minority among total HIV DNA (median: 12%) and became predominant thereafter (median at AIDS stage: 100%). Both total and integrated HIV DNA increased over a six-year period. Patients from the progression cohort who reached clinical AIDS during follow-up (n = 34) exhibited higher total and integrated HIV DNA levels at seroconversion and a higher percentage of integrated forms than did slower progressors (n = 63) (median: 100% vs 44%). The integrated HIV DNA load was strongly associated with the risk of developing AIDS (aRR = 2.63, p = 0.002).
Interpretation: The profile of "rapid" or "slower" progression in the natural history of HIV infection appears to be determined early in the course of HIV infection. The strong predominance of unstable unintegrated forms in PHI may explain the great benefit of this early treatment, which induces a sharp decrease in total HIV DNA. FUND: French National Agency for Research on AIDS and Viral Hepatitis.
Keywords: Acquired immunodeficiency syndrome; Integrated HIV DNA; Kinetics; Natural history; Primary HIV infection; Reservoirs; Total HIV DNA.
Copyright © 2019 The Authors. Published by Elsevier B.V. All rights reserved.
Figures



References
-
- Churchill M.J., Deeks S.G., Margolis D.M., Siliciano R.F., Swanstrom R. HIV reservoirs: what, where and how to target them. Nat Rev Microbiol. 2016;14(1):55–60. - PubMed
-
- Avettand-Fenoel V., Chaix M.L., Blanche S. LTR real-time PCR for HIV-1 DNA quantitation in blood cells for early diagnosis in infants born to seropositive mothers treated in HAART area (ANRS CO 01) J Med Virol. 2009;81(2):217–223. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
