

Variability in reported physician practices for brain death determination
- PMID: 30804063
- PMCID: PMC7987866
- DOI: 10.1212/WNL.0000000000007009
Variability in reported physician practices for brain death determination
Abstract
Objectives: The degree of training and variability in the clinical brain death examination performed by physicians is not known.
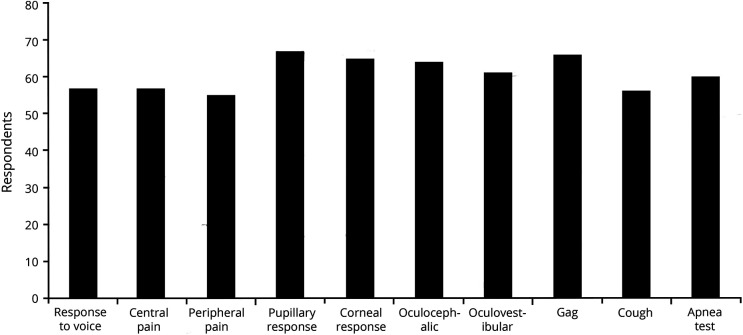
Methods: Surveys were distributed to physicians (including physicians-in-training) practicing at 3 separate academic medical centers. Data, including level of practice, training received in completion of a brain death examination, examination components performed, and use of confirmatory tests were collected. Data were evaluated for accuracy in the brain death examination, self-perceived competence in the examination, and indications for confirmatory tests.
Results: Of 225 total respondents, 68 reported completing brain death examinations in practice. Most physicians who complete a brain death examination reported they had received training in how to complete the examination (76.1%). Seventeen respondents (25%) reported doing a brain death examination that is consistent with the current practice guideline. As a part of their brain death assessment, 10.3% of physicians did not report completing an apnea test. Of clinicians who obtain confirmatory tests on an as-needed basis, 28.3% do so if a patient breathes during an apnea test, a clinical finding that is not consistent with brain death.
Conclusions: There is substantial variability in how physicians approach the adult brain death examination, but our survey also identified lack of training in nearly 1 in 4 academic physicians. A formal training course in the principles and proper technique of the brain death examination by physicians with expert knowledge of this clinical assessment is recommended.
© 2019 American Academy of Neurology.
Figures


Comment in
-
Strategies to improve uniformity in brain death determination.Neurology. 2019 Feb 26;92(9):401-402. doi: 10.1212/WNL.0000000000006994. Epub 2019 Jan 25. Neurology. 2019. PMID: 30804052 No abstract available.
-
Reader response: Variability in reported physician practices for brain death determination.Neurology. 2020 Jan 14;94(2):96-97. doi: 10.1212/WNL.0000000000008790. Neurology. 2020. PMID: 31932404 No abstract available.
-
Reader response: Variability in reported physician practices for brain death determination.Neurology. 2020 Jan 14;94(2):97. doi: 10.1212/WNL.0000000000008792. Neurology. 2020. PMID: 31932405 No abstract available.
-
Author response: Variability in reported physician practices for brain death determination.Neurology. 2020 Jan 14;94(2):98. doi: 10.1212/WNL.0000000000008788. Neurology. 2020. PMID: 31932406 No abstract available.
References
-
- Practice parameters for determining brain death in adults (summary statement): the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 1995;45:1012–1014. - PubMed
-
- Wijdicks EF, Varelas PN, Gronseth GS, Greer DM; American Academy of Neurology. Evidence-based guideline update: determining brain death in adults: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2010;74:1911–1918. - PubMed
-
- Greer DM, Wang HH, Robinson JD, Varelas PN, Henderson GV, Wijdicks EF. Variability of brain death policies in the United States. JAMA Neurol 2016;73:213–218. - PubMed
-
- Braksick SA, Kashani K, Hocker S. Neurology education for critical care fellows using high-fidelity simulation. Neurocrit Care 2017;26:96–102. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials