

A single dose of neoadjuvant PD-1 blockade predicts clinical outcomes in resectable melanoma
- PMID: 30804515
- PMCID: PMC6699626
- DOI: 10.1038/s41591-019-0357-y
A single dose of neoadjuvant PD-1 blockade predicts clinical outcomes in resectable melanoma
Abstract
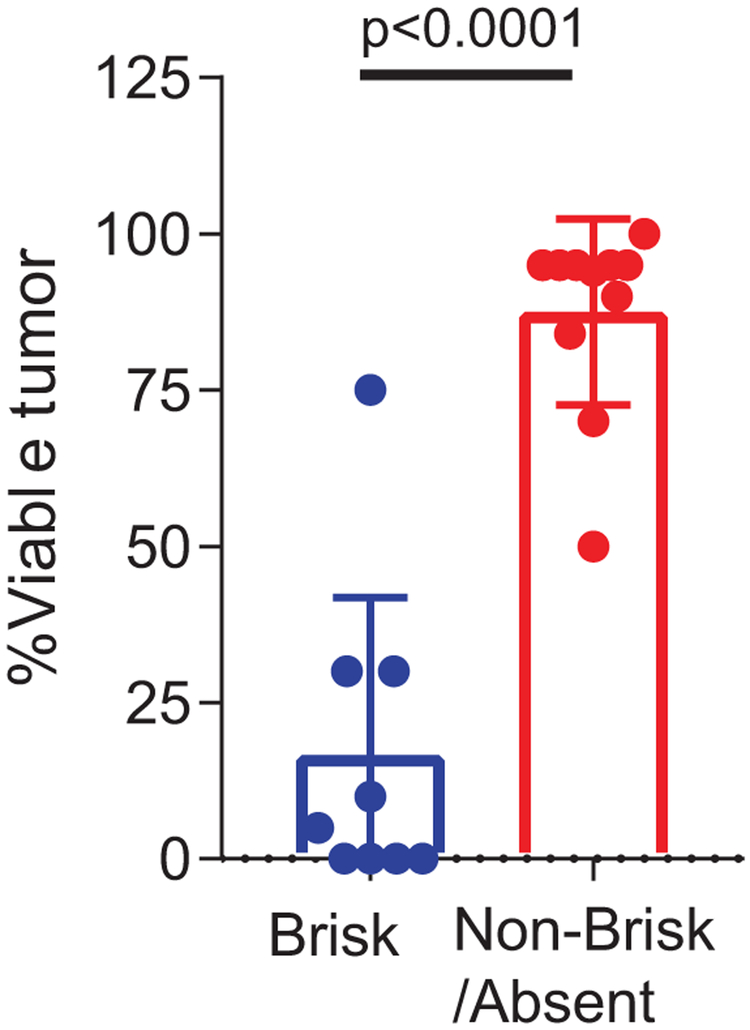
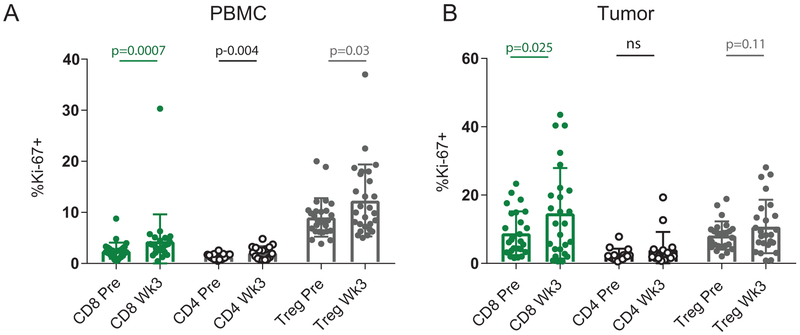
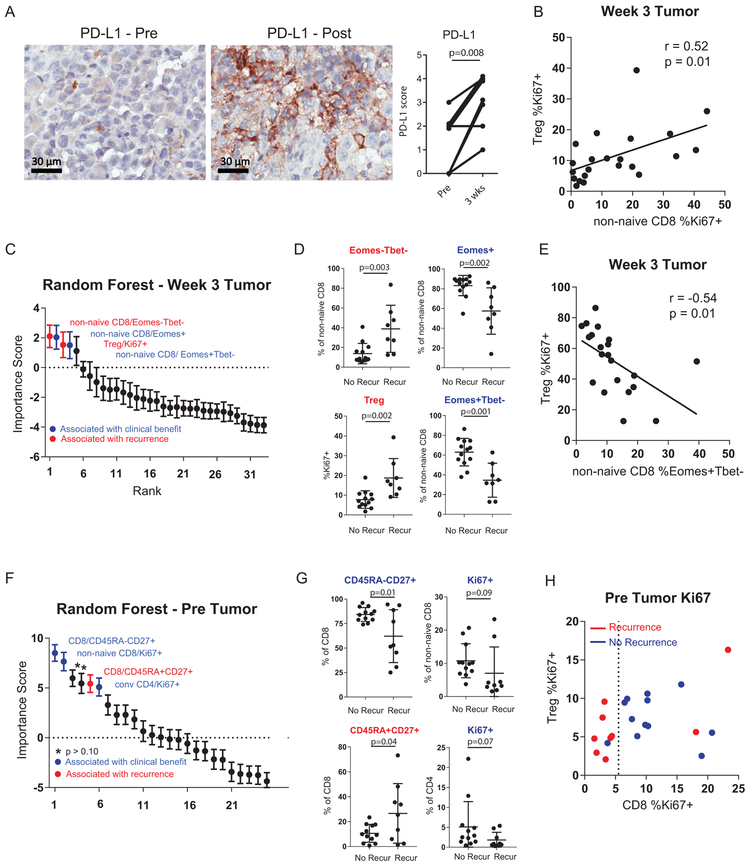
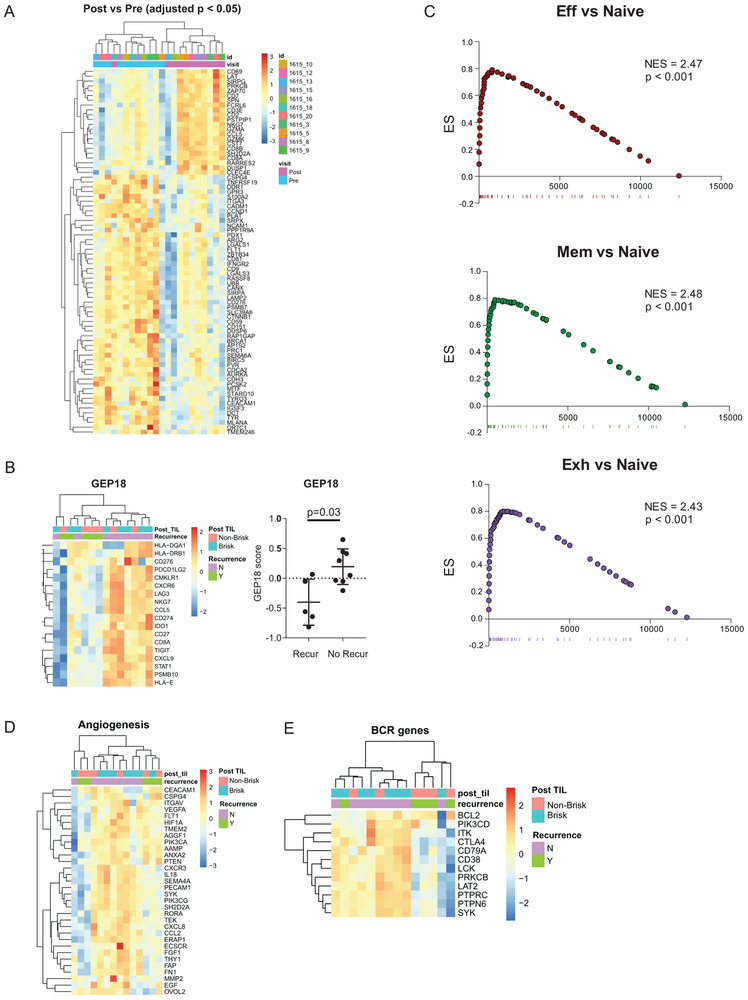
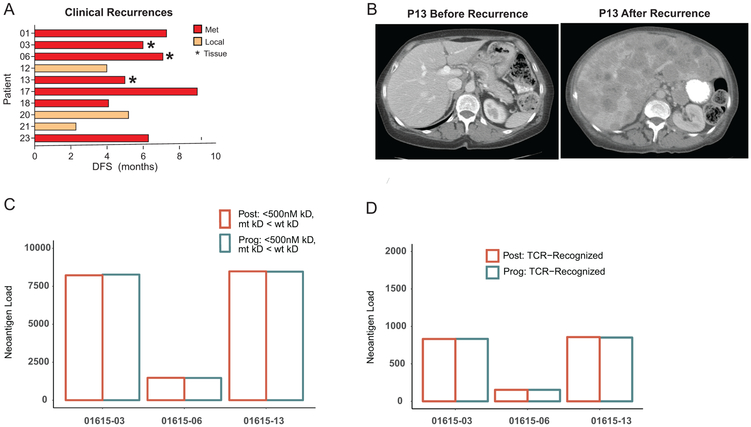
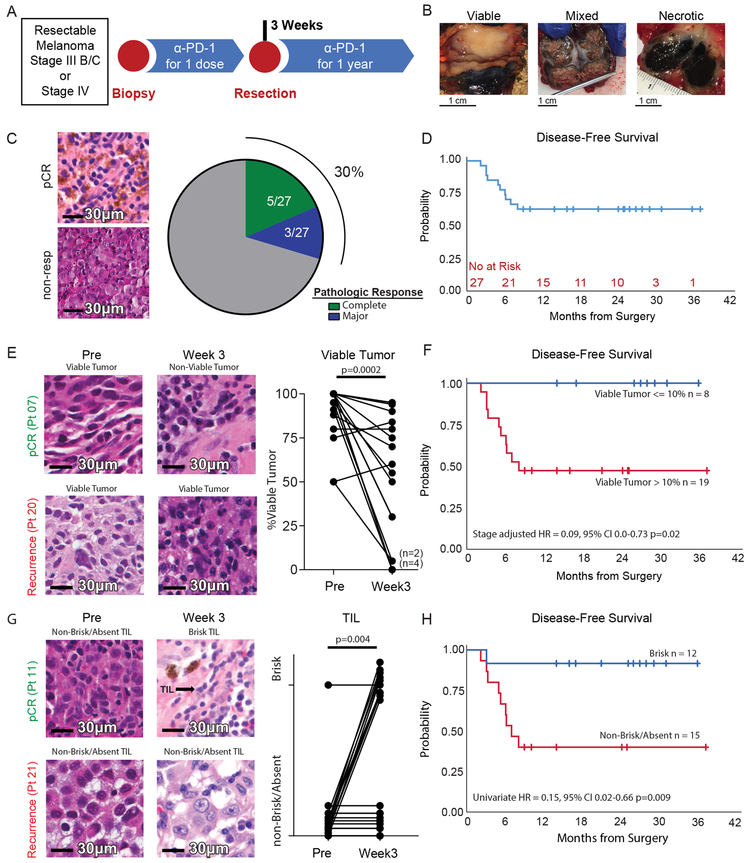
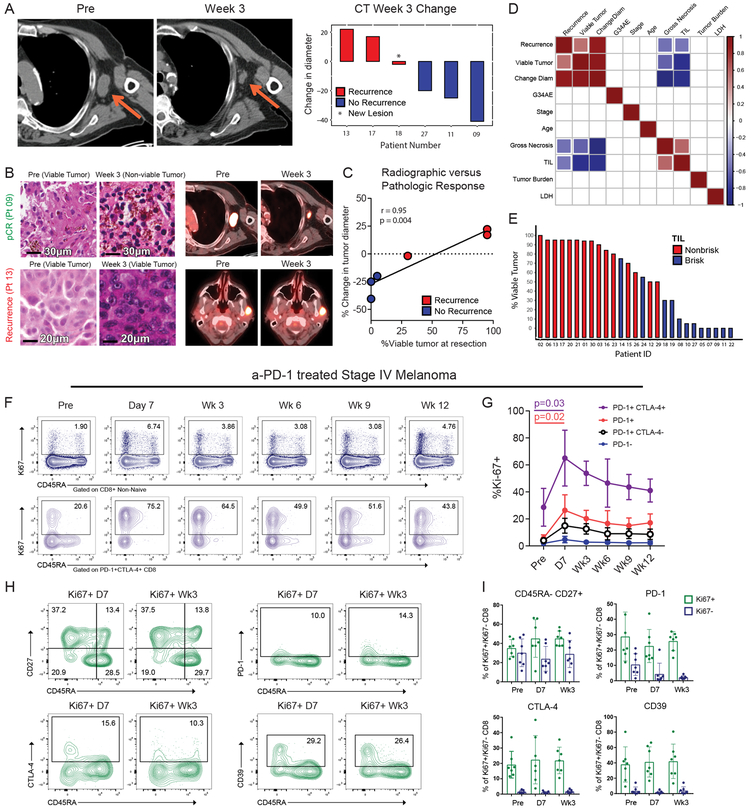
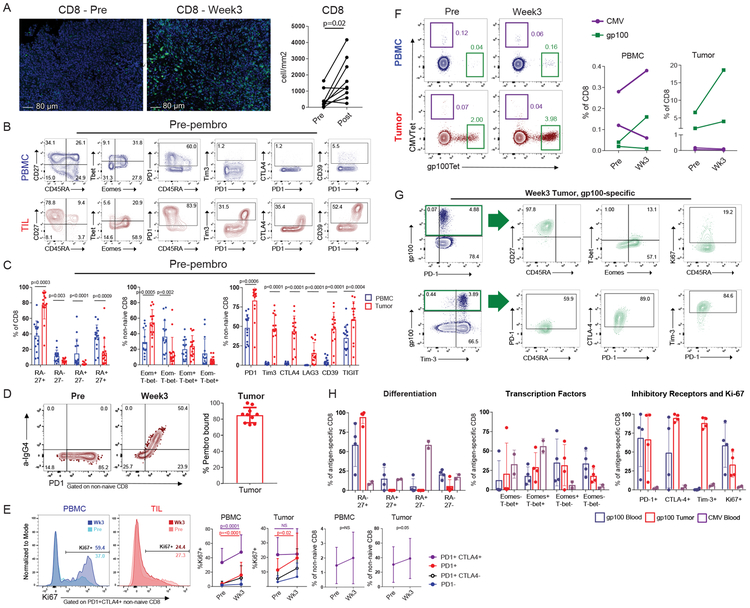
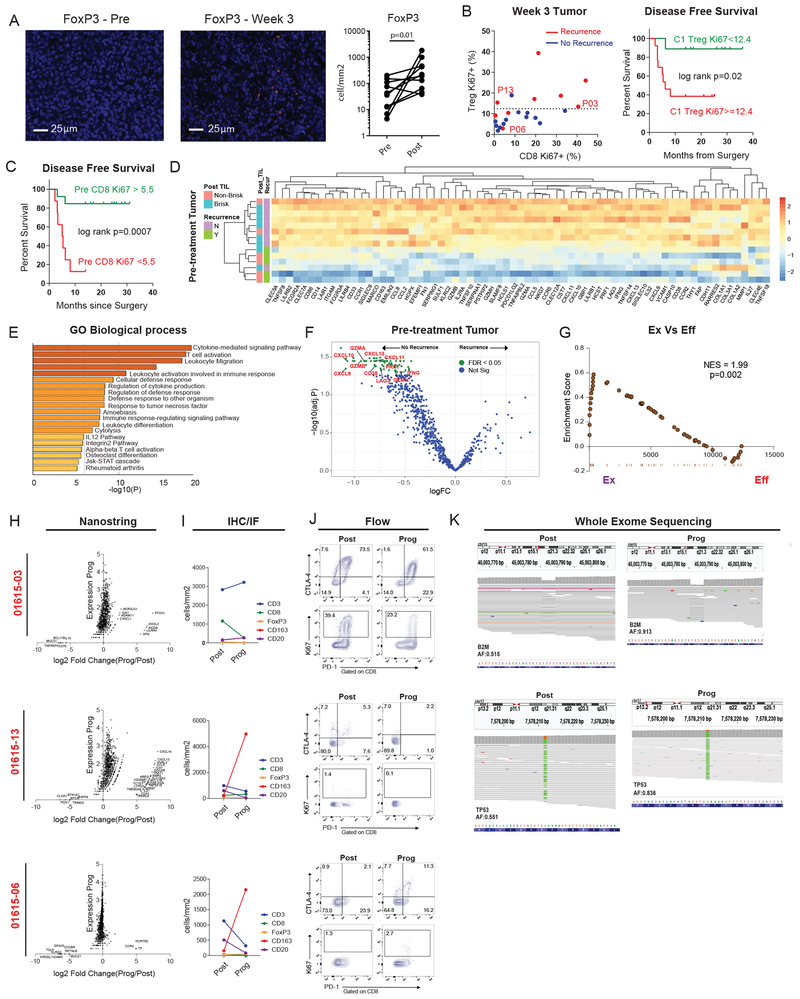
Immunologic responses to anti-PD-1 therapy in melanoma patients occur rapidly with pharmacodynamic T cell responses detectable in blood by 3 weeks. It is unclear, however, whether these early blood-based observations translate to the tumor microenvironment. We conducted a study of neoadjuvant/adjuvant anti-PD-1 therapy in stage III/IV melanoma. We hypothesized that immune reinvigoration in the tumor would be detectable at 3 weeks and that this response would correlate with disease-free survival. We identified a rapid and potent anti-tumor response, with 8 of 27 patients experiencing a complete or major pathological response after a single dose of anti-PD-1, all of whom remain disease free. These rapid pathologic and clinical responses were associated with accumulation of exhausted CD8 T cells in the tumor at 3 weeks, with reinvigoration in the blood observed as early as 1 week. Transcriptional analysis demonstrated a pretreatment immune signature (neoadjuvant response signature) that was associated with clinical benefit. In contrast, patients with disease recurrence displayed mechanisms of resistance including immune suppression, mutational escape, and/or tumor evolution. Neoadjuvant anti-PD-1 treatment is effective in high-risk resectable stage III/IV melanoma. Pathological response and immunological analyses after a single neoadjuvant dose can be used to predict clinical outcome and to dissect underlying mechanisms in checkpoint blockade.
Figures
Comment in
-
Early responses indicate remission.Nat Rev Clin Oncol. 2019 May;16(5):272. doi: 10.1038/s41571-019-0196-2. Nat Rev Clin Oncol. 2019. PMID: 30837713 No abstract available.
References
-
- Fridman WH, Pages F, Sautes-Fridman C & Galon J The immune contexture in human tumours: impact on clinical outcome. Nat Rev Cancer 12, 298–306 (2012). - PubMed
-
- Vesely MD, Kershaw MH, Schreiber RD & Smyth MJ Natural innate and adaptive immunity to cancer. Annu Rev Immunol 29, 235–271 (2011). - PubMed
-
- Simoni Y, et al. Bystander CD8(+) T cells are abundant and phenotypically distinct in human tumour infiltrates. Nature 557, 575–579 (2018). - PubMed
Methods-Only References
-
- Mihm MC Jr., Clemente CG & Cascinelli N Tumor infiltrating lymphocytes in lymph node melanoma metastases: a histopathologic prognostic indicator and an expression of local immune response. Lab Invest 74, 43–47 (1996). - PubMed
-
- Heinze G & Schemper M A solution to the problem of monotone likelihood in Cox regression. Biometrics 57, 114–119 (2001). - PubMed
-
- Chen M, et al. Development and validation of a novel clinical fluorescence in situ hybridization assay to detect JAK2 and PD-L1 amplification: a fluorescence in situ hybridization assay for JAK2 and PD-L1 amplification. Mod Pathol 30, 1516–1526 (2017). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
