

Pediatric localized intestinal lymphangiectasia treated with resection
- PMID: 30804688
- PMCID: PMC6375111
- DOI: 10.2147/IMCRJ.S192940
Pediatric localized intestinal lymphangiectasia treated with resection
Abstract
Introduction: Primary intestinal lymphangiectasia (PIL) is a very rare disorder usually diagnosed before the third year of life or later in adulthood, presenting with pitting edema, hypoproteinemia and low immunoglobulin levels. The location and the extent of the affected bowel greatly influence the clinical manifestation. The localized or segmental form of PIL is extremely rare with only five pediatric cases reported worldwide.
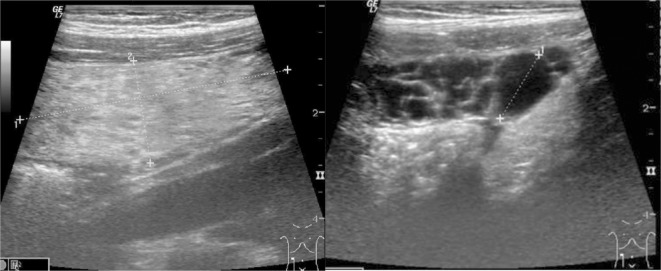
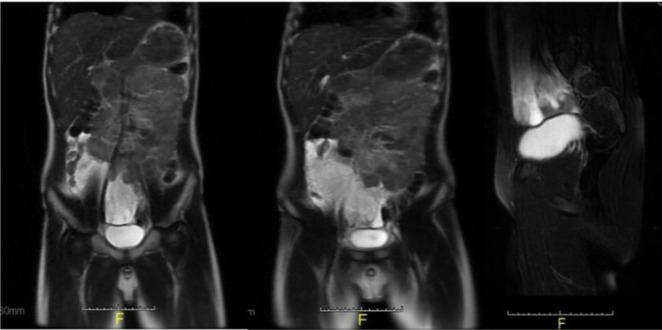
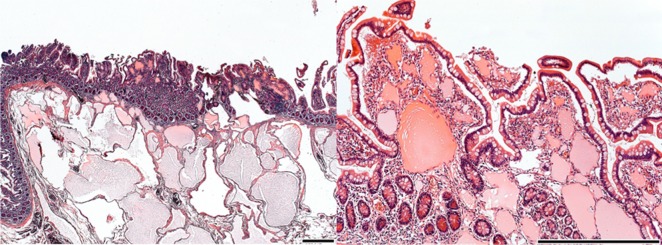
Case presentation: A 10 year-old Caucasian boy presented with 3 months history of recurrent abdominal pain and a 1 month history of diarrhea. An ultrasound scan was performed on two separate occasions 10 days apart, revealing a growing cystic mass on the right side of the abdomen, in front of the psoas muscle. Subsequently an MRI scan confirmed that the mass originated from the mesenteries and infiltrates a short segment of the small bowel. Surgical resection of the affected segment was performed. Histopathological examination of the removed segment of ileum was consistent with intestinal lymphangiectasia. We could not identify any associated genetic syndromes or any other conditions that could have caused secondary intestinal lymphangiectasia. The patient's recovery from surgery was uneventful and no recurrence was observed in the following 4 years.
Conclusion: Despite being a benign condition, mortality of PIL can be as high as 13% due to the difficulties associated with the management of the disease. PIL should be considered as a rare but potential cause for an abdominal mass, even in the older child, when cystic mesenterial involvement might be seen on ultrasound or MRI. In selected cases of PIL affecting only a short segment of the bowel or following unsuccessful conservative treatment, surgical resection of the affected bowel segment can be curative.
Keywords: abdominal mass; abdominal pain; children; follow-up; surgery.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures
Similar articles
-
Misty mesentery, ascites, and bowel wall thickening in a child: Diagnostic clue for intestinal lymphangiectasia.Radiol Case Rep. 2023 Sep 2;18(11):4032-4035. doi: 10.1016/j.radcr.2023.08.034. eCollection 2023 Nov. Radiol Case Rep. 2023. PMID: 37680662 Free PMC article.
-
Primary intestinal lymphangiectasia (Waldmann's disease).Orphanet J Rare Dis. 2008 Feb 22;3:5. doi: 10.1186/1750-1172-3-5. Orphanet J Rare Dis. 2008. PMID: 18294365 Free PMC article. Review.
-
Primary intestinal lymphangiectasia in an adult patient: A case report and review of literature.World J Gastroenterol. 2020 Dec 28;26(48):7707-7718. doi: 10.3748/wjg.v26.i48.7707. Epub 2020 Dec 8. World J Gastroenterol. 2020. PMID: 33505146 Free PMC article. Review.
-
Primary intestinal lymphangiectasia diagnosed by capsule endoscopy and double balloon enteroscopy.World J Gastrointest Endosc. 2011 Nov 16;3(11):235-40. doi: 10.4253/wjge.v3.i11.235. World J Gastrointest Endosc. 2011. PMID: 22110841 Free PMC article.
-
Primary Intestinal Lymphangiectasia Manifested as Unusual Edemas and Effusions: A Case Report.Medicine (Baltimore). 2016 Mar;95(10):e2849. doi: 10.1097/MD.0000000000002849. Medicine (Baltimore). 2016. PMID: 26962779 Free PMC article.
Cited by
-
Pathophysiology, Diagnosis, and Management of Canine Intestinal Lymphangiectasia: A Comparative Review.Animals (Basel). 2022 Oct 15;12(20):2791. doi: 10.3390/ani12202791. Animals (Basel). 2022. PMID: 36290177 Free PMC article. Review.
-
Small intestinal mucosal abnormalities using video capsule endoscopy in intestinal lymphangiectasia.Orphanet J Rare Dis. 2023 Oct 2;18(1):308. doi: 10.1186/s13023-023-02914-z. Orphanet J Rare Dis. 2023. PMID: 37784188 Free PMC article.
-
Individual approach for treatment of primary intestinal lymphangiectasia in children: single-center experience and review of the literature.BMC Pediatr. 2021 Jan 7;21(1):21. doi: 10.1186/s12887-020-02447-5. BMC Pediatr. 2021. PMID: 33407260 Free PMC article. Review.
References
-
- Levine C. Primary disorders of the lymphatic vessels—a unified concept. J Pediatr Surg. 1989;24(3):233–240. - PubMed
-
- Hokari R, Kitagawa N, Watanabe C, et al. Changes in regulatory molecules for lymphangiogenesis in intestinal lymphangiectasia with enteric protein loss. J Gastroenterol Hepatol. 2008;23(7 Pt 2):e88–e95. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
