

Apraclonidine Is Better Than Cocaine for Detection of Horner Syndrome
- PMID: 30804875
- PMCID: PMC6371044
- DOI: 10.3389/fneur.2019.00055
Apraclonidine Is Better Than Cocaine for Detection of Horner Syndrome
Abstract
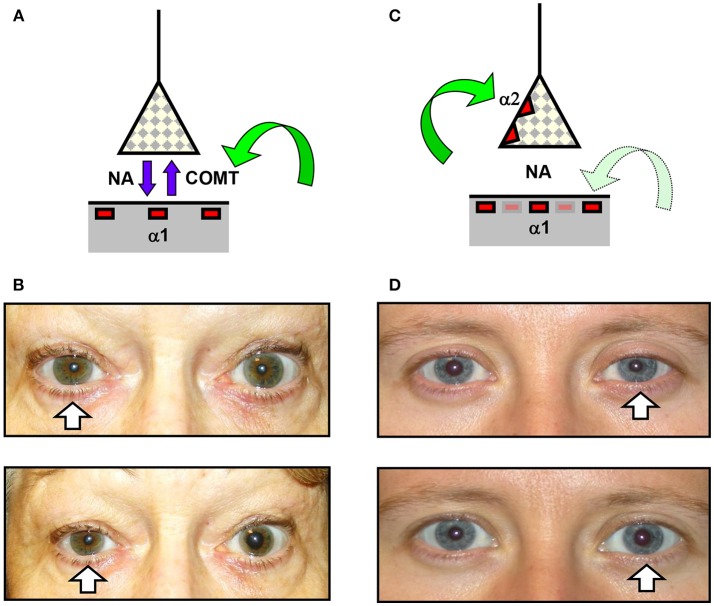
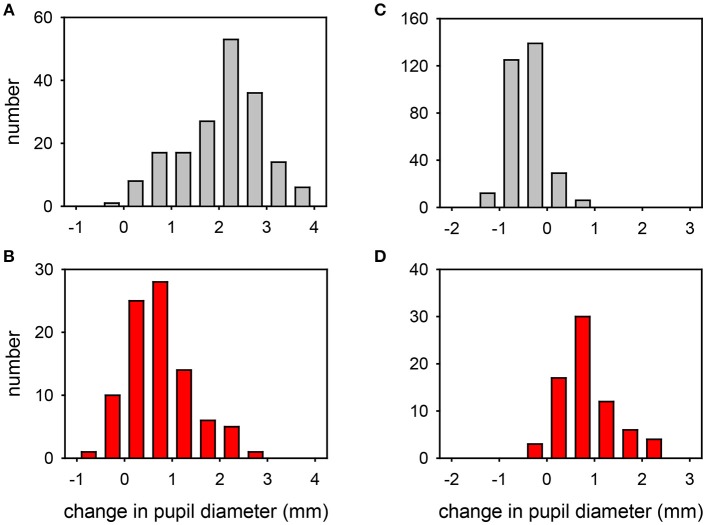
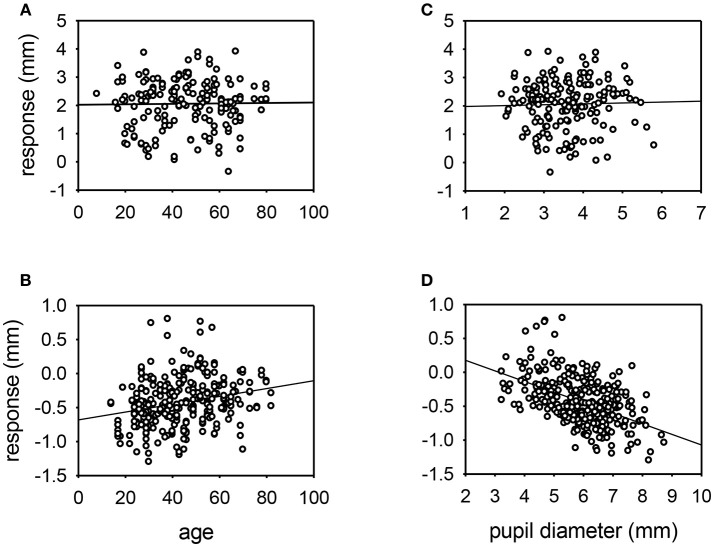
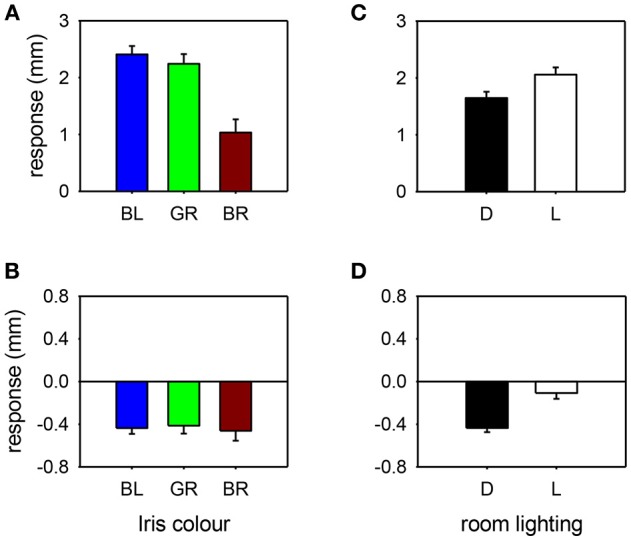
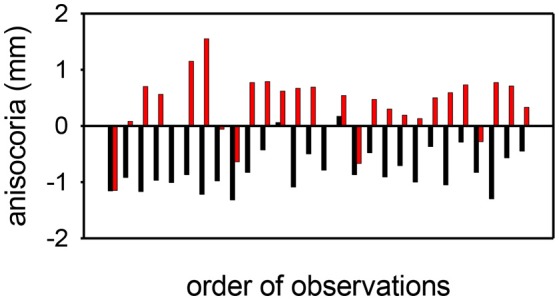
Background: In suspected cases of Horner syndrome pharmacological confirmation is often required before embarking on further investigations. There are two drugs currently used for this purpose that are commercially available for topical administration: cocaine (2-10%) and apraclonidine (0.5-1.0%). Aims: To evaluate and compare the effects of both drugs in normal eyes and eyes with Horner syndrome Methods: This is a retrospective study looking at the outcome of 660 consecutive pharmacological tests with these two drugs in one tertiary referral center over 14 years. Eyes were categorized as "normal" or "Horner syndrome" based on non-pharmacological criteria (pupillometric and clinical evidence). Pupil diameters in the dark and in bright light were measured by pupillometry before and 40 min after administration of the test drug (either 4% cocaine or 0.5% apraclonidine). Results: Cocaine dilated the normal pupil (measured in bright light: mean +2.1 mm, range -0.4 to +3.9 mm; 95% lower limit +0.5 mm); the extent of this response was not significantly affected by patient age or pupil size, but was 50% less in brown eyes compared with blue or green eyes, and 20% less if the measurements were made in the dark. In eyes with Horner syndrome cocaine had significantly less mydriatic effect (mean +0.7 mm, range -0.7 to +2.9 mm). Apraclonidine constricted the normal pupil (measured in the dark: mean -0.4 mm, range -1.3 to +0.8 mm; 95% upper limit +0.1 mm); eye color made no difference but the response was significantly greater in younger patients and larger pupils and significantly less if measured in bright lighting conditions. In eyes with Horner syndrome apraclonidine dilated the pupil (mean +0.6, range -0.4 to +2.3 mm). Applying the 95% limits identified from my normative data, I estimate the sensitivity of each drug test for detection of Horner syndrome at 40% for cocaine (criterion for abnormal: mydriasis ≤0.5 mm when measured in the dark) compared with 93% for apraclonidine (criterion for abnormal: mydriasis ≥0.1 mm when measured in the dark). Conclusions: Apraclonidine is a more sensitive test than cocaine for detection of Horner syndrome, and should be adopted as the new gold standard in routine clinical practice. However, caution is needed when using this drug within hours of a suspected sympathetic lesion, or in infants under 1 year of age.
Keywords: Horner syndrome; apraclonidine; cocaine; pharmacological testing; pupillometry; test sensitivity.
Figures

References
-
- Horner JF. On a form of ptosis. Klin Monatsbl Augenheilk. (1869) 7:193–8.
LinkOut - more resources
Full Text Sources