

Incidence of community onset MRSA in Australia: least reported where it is Most prevalent
- PMID: 30805180
- PMCID: PMC6373119
- DOI: 10.1186/s13756-019-0485-7
Incidence of community onset MRSA in Australia: least reported where it is Most prevalent
Abstract
Background: This is the first review of literature and synthesis of data on community onset methicillin resistant Staphylococcus aureus (CO-MRSA) infections in Australia. Incidence of CO-MRSA varies considerably in Australia, depending on geographic and demographic factors.
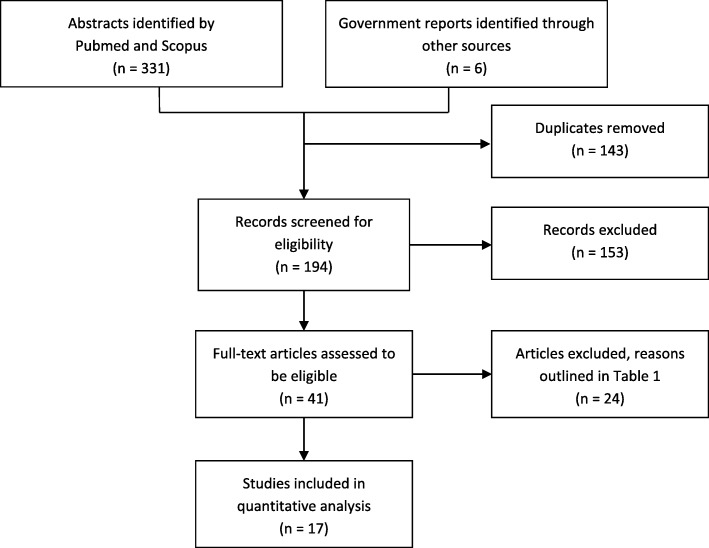
Methods: Data for the rates of MRSA infections were collected from articles identified using PubMed, Scopus, the grey literature and data from State and Federal Government Surveillance Systems. We synthesized data and developed a framework for how data was selected, collated, linked, organized and interpreted.
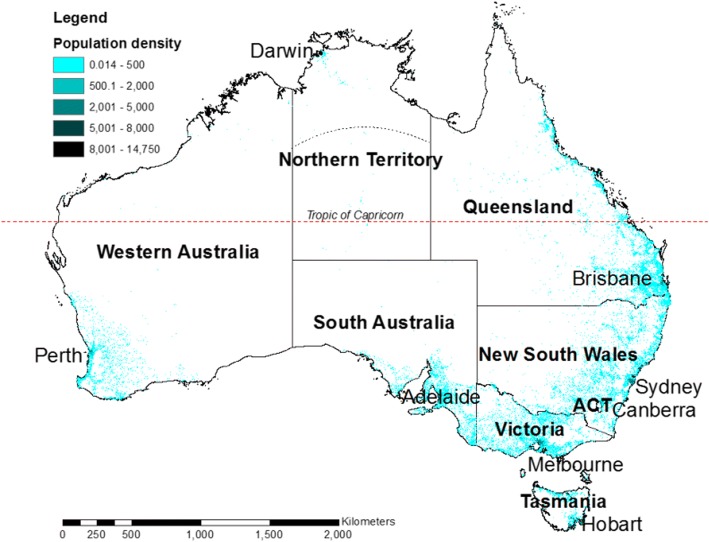
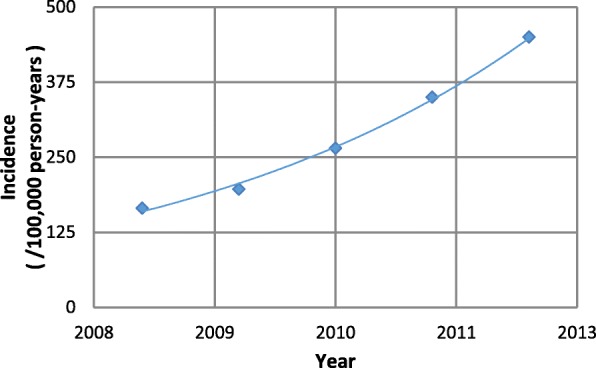
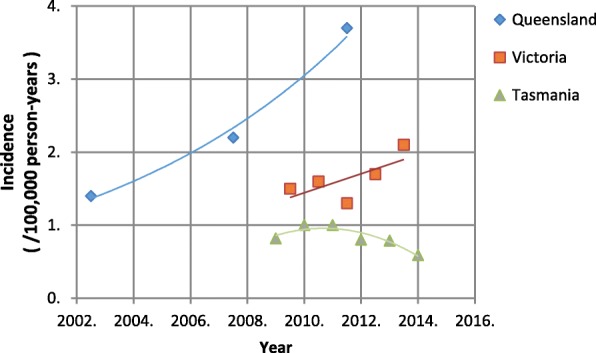
Results: The results of our literature search demonstrates considerable gaps in the reporting of CO-MRSA in Australia. Consequently, total incidences were under reported; however the available data suggests the incidence varied between 44 (Tasmania) and 388 (southern Northern Territory) cases per 100,000 person years. Hospitalised cases of CO-MRSA varied between 3.8 (regional Victoria) and 329 (southern Northern Territory). Taking the median percentage of infections by site for all regions available, skin and soft tissue infections (SSTIs) consisted of 56% of hospitalized CO-MRSA, compared with bacteremias, which represented 14%. No region had a complete data set of CO-MRSA infections treated in out-patient settings and so incidences were underestimates. Nevertheless, estimates of the incidence of CO-MRSA treated outside hospitals varied between 11.3 (Melbourne) and 285 (Northern Territory) per 100,000 person-years. These infections were chiefly SSTIs, although urinary tract infections were also noted.Incidences of CO-MRSA blood-stream infections and outpatient skin and soft tissue infections have been increasing with time, except in Tasmania. CO-MRSA is observed to affect people living in remote areas and areas of socioeconomic disadvantage disproportionately.
Conclusions: We generated the first estimates of the incidence of CO-MRSA infections in Australia and identified stark regional differences in the nature and frequency of infections. Critically, we demonstrate that there has been a lack of consistency in reporting CO-MRSA and a general dearth of data. The only government in Australia that requires reporting of CO-MRSA is the Tasmanian, where the infection was least prevalent. Some regions of Australia have very high incidences of CO-MRSA. To improve surveillance and inform effective interventions, we recommend a standardized national reporting system in Australia that reports infections at a range of infection sites, has broad geographic coverage and consistent use of terminology. We have identified limitations in the available data that hinder understanding the prevalence of CO-MRSA.
Keywords: Antimicrobial resistance; Australia; Community; Methicillin resistant Staphylococcus aureus; Staphylococcus aureus.
Conflict of interest statement
Not applicable.Not applicable.The authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
High burden of complicated skin and soft tissue infections in the Indigenous population of Central Australia due to dominant Panton Valentine leucocidin clones ST93-MRSA and CC121-MSSA.BMC Infect Dis. 2017 Jun 7;17(1):405. doi: 10.1186/s12879-017-2460-3. BMC Infect Dis. 2017. PMID: 28592231 Free PMC article.
-
The rise of methicillin resistant Staphylococcus aureus: now the dominant cause of skin and soft tissue infection in Central Australia.Epidemiol Infect. 2017 Oct;145(13):2817-2826. doi: 10.1017/S0950268817001716. Epub 2017 Aug 14. Epidemiol Infect. 2017. PMID: 28803587 Free PMC article.
-
Epidemiology of Staphylococcus aureus blood and skin and soft tissue infections in the US military health system, 2005-2010.JAMA. 2012 Jul 4;308(1):50-9. doi: 10.1001/jama.2012.7139. JAMA. 2012. PMID: 22760291
-
Methicillin-resistant Staphylococcus aureus: an overview of basic and clinical research.Nat Rev Microbiol. 2019 Apr;17(4):203-218. doi: 10.1038/s41579-018-0147-4. Nat Rev Microbiol. 2019. PMID: 30737488 Free PMC article. Review.
-
Invasive community-associated MRSA infections: epidemiology and antimicrobial management.Expert Opin Pharmacother. 2010 Dec;11(18):3009-25. doi: 10.1517/14656566.2010.511614. Epub 2010 Oct 19. Expert Opin Pharmacother. 2010. PMID: 20955116 Review.
Cited by
-
Antimicrobial stewardship in rural and remote primary health care: a narrative review.Antimicrob Resist Infect Control. 2021 Jul 13;10(1):105. doi: 10.1186/s13756-021-00964-1. Antimicrob Resist Infect Control. 2021. PMID: 34256853 Free PMC article. Review.
-
The antibacterial effectiveness of lavender essential oil against methicillin-resistant Staphylococcus aureus: a systematic review.Front Pharmacol. 2023 Dec 7;14:1306003. doi: 10.3389/fphar.2023.1306003. eCollection 2023. Front Pharmacol. 2023. PMID: 38130406 Free PMC article.
-
Efficacy and Safety of Intravenous Lincosamide Therapy in Methicillin-Resistant Staphylococcus aureus Bacteremia.Antimicrob Agents Chemother. 2021 Aug 17;65(9):e0034321. doi: 10.1128/AAC.00343-21. Epub 2021 Aug 17. Antimicrob Agents Chemother. 2021. PMID: 34125589 Free PMC article.
-
Trends in clinical management of lactational mastitis among women attending Australian general practice: a national longitudinal study using MedicineInsight, 2011-2022.BMJ Open. 2024 May 20;14(5):e080128. doi: 10.1136/bmjopen-2023-080128. BMJ Open. 2024. PMID: 38772591 Free PMC article.
-
Optimization of Fermentation Conditions for Endophytic Fungi from Schisandra chinensis and Investigation of Their Antibacterial Mechanisms Against Methicillin-Resistant Staphylococcus aureus.Microorganisms. 2025 Apr 25;13(5):982. doi: 10.3390/microorganisms13050982. Microorganisms. 2025. PMID: 40431155 Free PMC article.
References
-
- Munckhof WJ, Nimmo GR, Schooneveldt JM, Schlebusch S, Stephens AJ, Williams G, et al. Nasal carriage of Staphylococcus aureus, including community-associated methicillin-resistant strains, in Queensland adults. Clin Microbiol Infect. 2009;15(2):149–155. - PubMed
-
- Stubbs E, Pegler M, Vickery A, Harbour C. Nasal carriage of Staphylococcus aureus in Australian (pre-clinical and clinical) medical students. J Hosp Infect. 1994;27(2):127–134. - PubMed
-
- Wertheim HFL, Melles DC, Vos MC, van Leeuwen W, van Belkum A, Verbrugh HA, et al. The role of nasal carriage in Staphylococcus aureus infections. Lancet Infect Dis. 2005;5(12):751–762. - PubMed
-
- Turnidge JD, Kotsanas D, Munckhof W, Roberts S, Bennett CM, Nimmo GR, et al. Staphylococcus aureus bacteraemia: a major cause of mortality in Australia and New Zealand. Med J Aust. 2009;191(7):368–373. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
