

Traumatic Fracture of the Pediatric Cervical Spine: Etiology, Epidemiology, Concurrent Injuries, and an Analysis of Perioperative Outcomes Using the Kids' Inpatient Database
- PMID: 30805288
- PMCID: PMC6383458
- DOI: 10.14444/6009
Traumatic Fracture of the Pediatric Cervical Spine: Etiology, Epidemiology, Concurrent Injuries, and an Analysis of Perioperative Outcomes Using the Kids' Inpatient Database
Abstract
Background: The study aimed to characterize trends in incidence, etiology, fracture types, surgical procedures, complications, and concurrent injuries associated with traumatic pediatric cervical fracture using a nationwide database.
Methods: The Kids' Inpatient Database (KID) was queried. Trauma cases from 2003 to 2012 were identified, and cervical fracture patients were isolated. Demographics, etiologies, fracture levels, procedures, complications, and concurrent injuries were assessed. The t-tests elucidated significance for continuous variables, and χ2 for categoric values. Logistic regressions identified predictors of spinal cord injury (SCI), surgery, any complication, and mortality. Level of significance was P < .05.
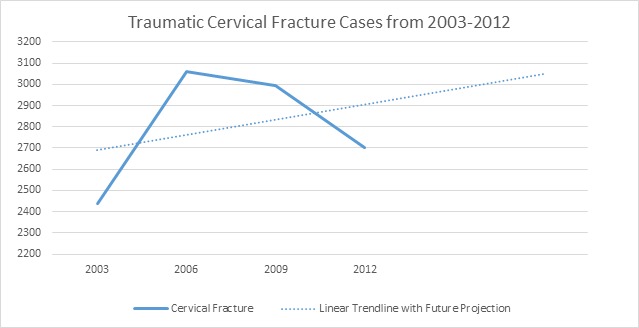
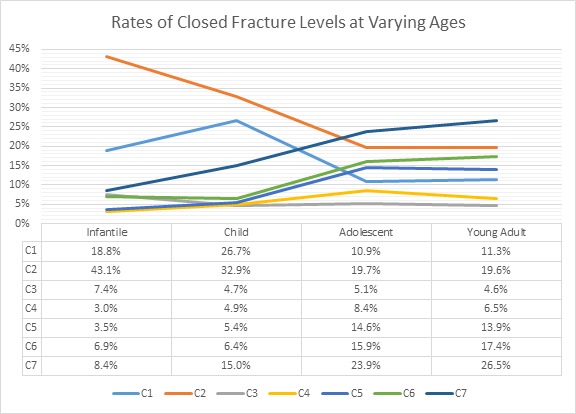
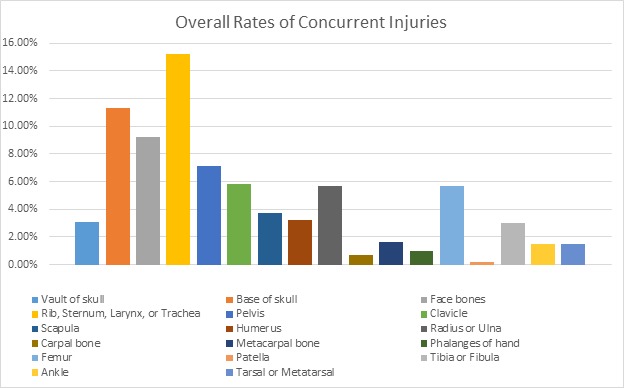
Results: A total of 11 196 fracture patients were isolated (age, 16.63 years; male, 65.7%; white, 65.4%; adolescent, 55.4%). Incidence significantly increased since 2003 (2003 vs 2012, 2.39% vs 3.12%, respectively), as did Charlson Comorbidity Index (CCI; 2003 vs 2012, 0.2012 vs 0.4408, respectively). Most common etiology was motor vehicle accidents (50.5%). Infants and children frequently fractured at C2 (closed: 43.1%, 32.9%); adolescents and young adults frequently fractured at C7 (closed: 23.9%, 26.5%). Upper cervical SCI was less common (5.8%) than lower cervical SCI (10.9%). Lower cervical unspecified-SCI, anterior cord syndrome, and other specified SCIs significantly decreased since 2003. Complications were common (acute respiratory distress syndrome, 7.8%; anemia, 6.7%; shock, 3.0%; and mortality, 4.2%), with bowel complications, cauda equina, anemia, and shock rates significantly increasing since 2003. Concurrent injuries were common (15.2% ribs; 14.4% skull; 7.1% pelvis) and have significantly increased since 2003. Predictors of SCI included sports injury and CCI. Predictors of surgery included falls, sports injuries, CCI, length of stay, and SCI. CCI, SCIs, and concurrent injuries were predictors of any complication and mortality, all (P < .001).
Conclusions: Since 2003, incidence, complications, concurrent injuries, and fusions have increased. CCI, SCI, falls, and sports injuries were significant predictors of surgical intervention. Decreased mortality and SCI rates may indicate improving emergency medical services and management guidelines.
Level of evidence: III.
Clinical relevance: Clinicians should be aware of increased case complexity in the onset of added perioperative complications and concurrent injuries. Cervical fractures resultant of sports injuries should be scrutinized for concurrent SCIs.
Keywords: cervical fracture; pediatrics; trauma.
Conflict of interest statement
Disclosures and COI: Dr Gerling received personal consulting fees for Paradigm Spine and speaking/teaching fees for Stryker Spine. Dr Passias received personal consulting fees for Spinewave and Medicrea. The other authors received no funding for this study and report no conflicts of interest.
Figures
References
-
- Osenbach RK, Menezes AH. Pediatric spinal cord and vertebral column injury. Neurosurgery. 1992;30(3):385–390. - PubMed
-
- Nitecki S, Moir CR. Predictive factors of the outcome of traumatic cervical spine fracture in children. J Pediatr Surg. 1994;29(11):1409–1411. - PubMed
-
- Eubanks JD, Gilmore A, Bess S, Cooperman DR. Clearing the pediatric cervical spine following injury. J Am Acad Orthop Surg. 2006;14(9):552–564. - PubMed
-
- Wakes S, Beukes A. Height, fun and safety in the design of children's playground equipment. Int J Inj Contr Saf Promot. 2012;19(2):101–108. - PubMed
-
- Gururaj G. Injury prevention and care: an important public health agenda for health, survival and safety of children. Indian J Pediatr. 2012;80(suppl 1):S100–S108. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous