

Cement augmentation of the proximal humerus internal locking system in elderly patients: a multicenter randomized controlled trial
- PMID: 30805708
- PMCID: PMC6570671
- DOI: 10.1007/s00402-019-03142-6
Cement augmentation of the proximal humerus internal locking system in elderly patients: a multicenter randomized controlled trial
Abstract
Introduction: Cement augmentation of the proximal humerus internal locking system (PHILOS) screws might reduce complication rates in osteoporotic bones. This study compared the risk of mechanical failure during the first year after PHILOS™ treatment of proximal humerus fractures (PHF) without (control group) and with (augmented group) screw augmentation. Secondary objectives were to report shoulder functions, quality of life (QoL), adverse events (AEs), and reoperation rates.
Materials and methods: This multicenter randomized trial enrolled patients aged ≥ 65 years with displaced/unstable PHF from eight European centers. Randomization was performed during surgery through sealed opaque envelopes. Mechanical failures were assessed by two independent reviewers via radiographs, shoulder function by Quick DASH, SPADI, and Constant Murley scores, and QoL by EQ-5D. Follow-ups were planned at postoperative 6 weeks, 3, 6, and 12 months.
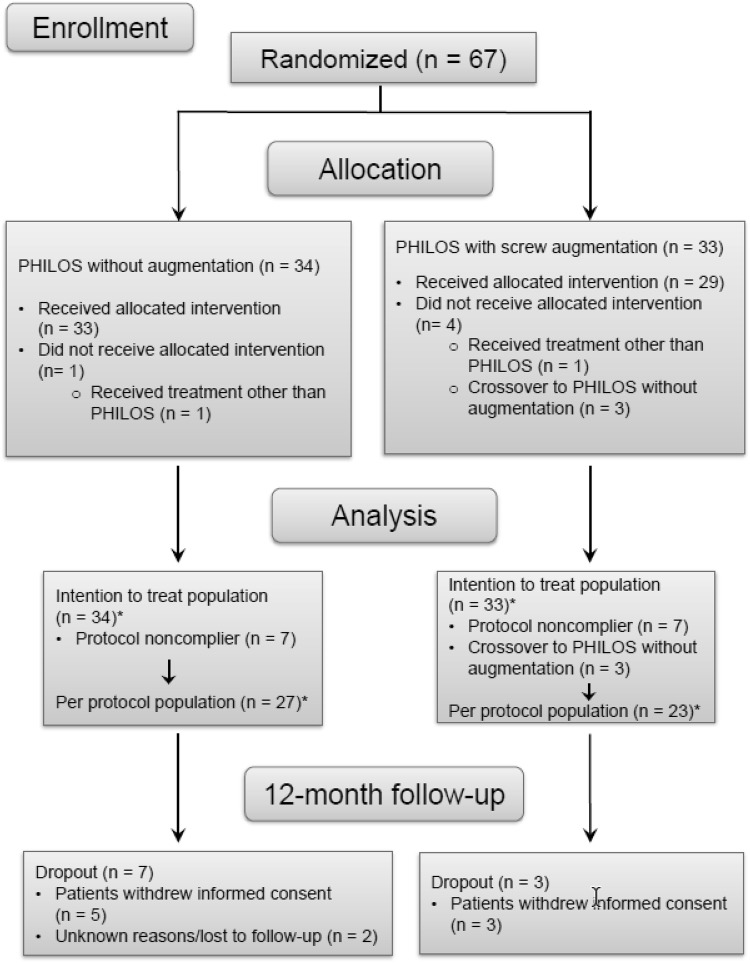
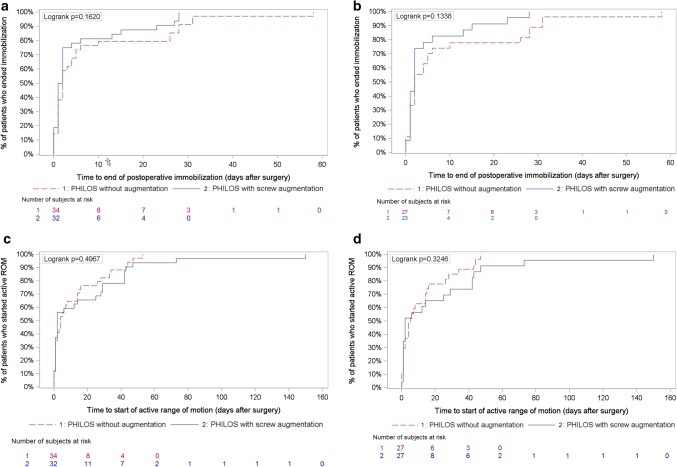
Results: The preliminary analysis of 6-week radiographs of the first 59 enrolled patients suggested a mechanical failure rate lower than expected and the difference between groups was too small to be detected by the planned sample size of 144. The trial was prematurely terminated after 67 patients had been enrolled: 34 (27 eligible) in the control group and 33 (29 eligible) in the augmented group. Follow-ups were performed as planned. Nine patients had mechanical failures and the failure rates (95% CI) were: augmented group, 16.1% (5.5; 33.7); control group, 14.8% (4.2; 33.7); the relative risk (95% CI) for the augmented group was 1.09 (0.32; 3.65) compared to the control group (p = 1.000). No statistically significant differences in shoulder function, QoL, and AEs were observed between study groups at 1 year. Nine patients (15.8%) underwent a revision.
Conclusions: Due to premature termination, the study was underpowered. A larger study will be necessary to determine if cement augmentation lowers the risk of mechanical failure rate.
Keywords: Augmentation; Multicenter randomized trial; Osteoporosis; PHILOS; Proximal humerus fracture; Proximal humerus internal locking system.
Conflict of interest statement
Franz Kralinger is a consultant with DePuySynthes but did not receive personal benefits for the current study. Tim Pohlemann was the chairman of the AO TK-System during the time of study. Martin Jaeger is a member of the AO UEEG.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
