

Rethinking interhemispheric imbalance as a target for stroke neurorehabilitation
- PMID: 30805956
- PMCID: PMC7374229
- DOI: 10.1002/ana.25452
Rethinking interhemispheric imbalance as a target for stroke neurorehabilitation
Abstract
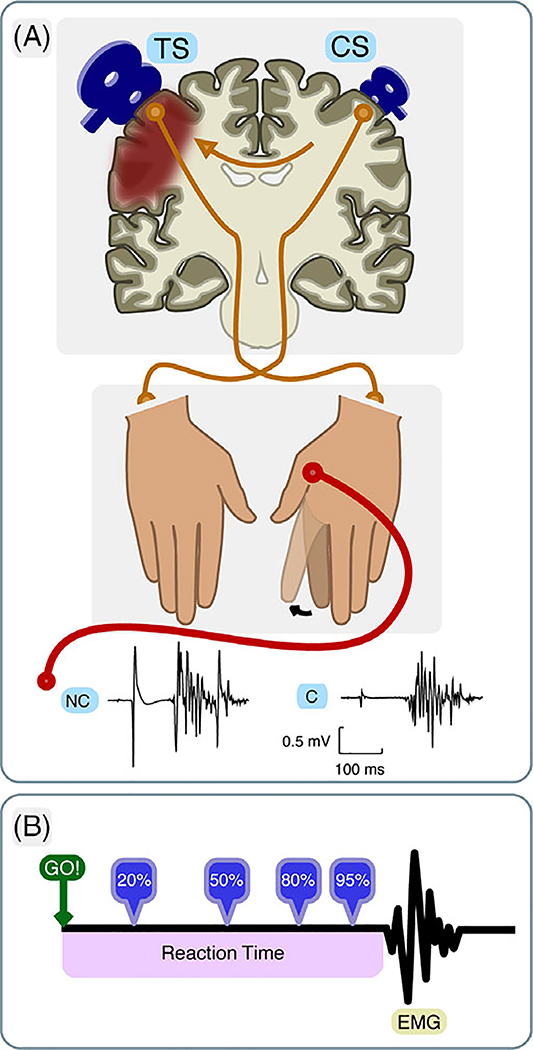
Objective: Patients with chronic stroke have been shown to have failure to release interhemispheric inhibition (IHI) from the intact to the damaged hemisphere before movement execution (premovement IHI). This inhibitory imbalance was found to correlate with poor motor performance in the chronic stage after stroke and has since become a target for therapeutic interventions. The logic of this approach, however, implies that abnormal premovement IHI is causal to poor behavioral outcome and should therefore be present early after stroke when motor impairment is at its worst. To test this idea, in a longitudinal study, we investigated interhemispheric interactions by tracking patients' premovement IHI for one year following stroke.
Methods: We assessed premovement IHI and motor behavior five times over a 1-year period after ischemic stroke in 22 patients and 11 healthy participants.
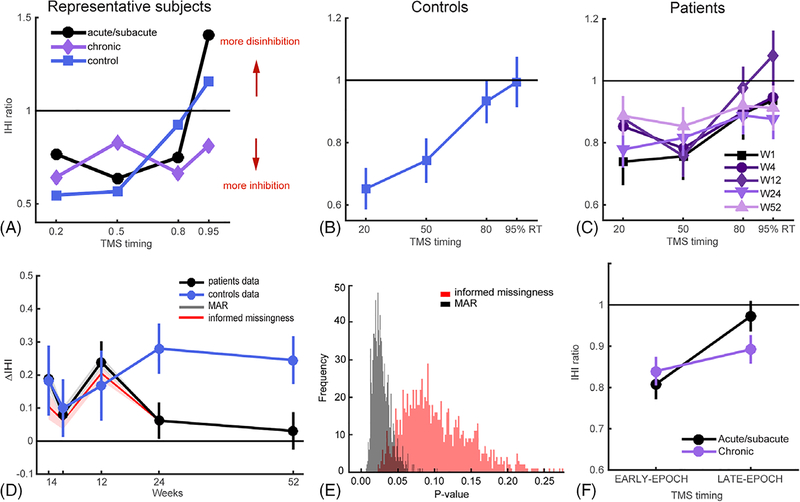
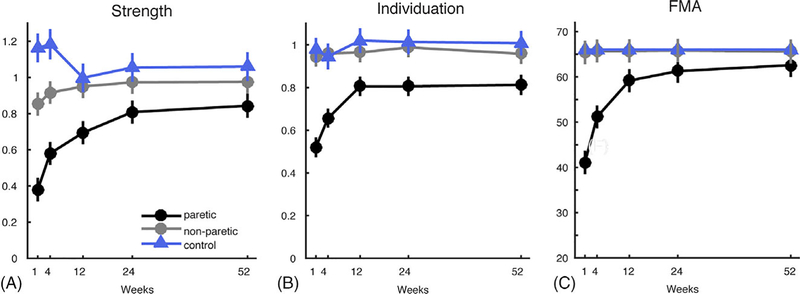
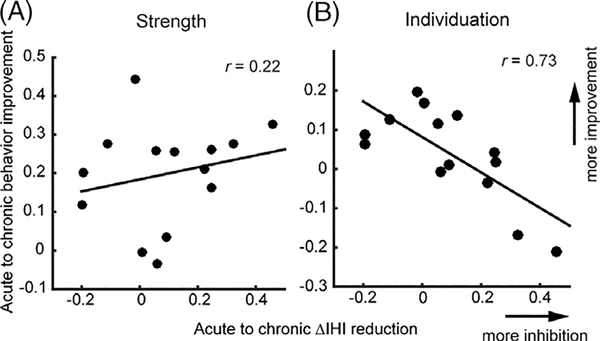
Results: We found that premovement IHI was normal during the acute/subacute period and only became abnormal at the chronic stage; specifically, release of IHI in movement preparation worsened as motor behavior improved. In addition, premovement IHI did not correlate with behavioral measures cross-sectionally, whereas the longitudinal emergence of abnormal premovement IHI from the acute to the chronic stage was inversely correlated with recovery of finger individuation.
Interpretation: These results suggest that interhemispheric imbalance is not a cause of poor motor recovery, but instead might be the consequence of underlying recovery processes. These findings call into question the rehabilitation strategy of attempting to rebalance interhemispheric interactions in order to improve motor recovery after stroke. Ann Neurol 2019;85:502-513.
© 2019 American Neurological Association.
Conflict of interest statement
Potential Conflicts of Interest
Nothing to report.
Figures
References
-
- Murase N, Duque J, Mazzocchio R, Cohen LG. Influence of interhemispheric interactions on motor function in chronic stroke. Ann Neurol 2004;55:400–409. - PubMed
-
- Hummel FC, Cohen LG. Non-invasive brain stimulation: a new strategy to improve neurorehabilitation after stroke? Lancet Neurol 2006; 5:708–712. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
