

Effect of Patient-Centered Transitional Care Services on Clinical Outcomes in Patients Hospitalized for Heart Failure: The PACT-HF Randomized Clinical Trial
- PMID: 30806695
- PMCID: PMC6439867
- DOI: 10.1001/jama.2019.0710
Effect of Patient-Centered Transitional Care Services on Clinical Outcomes in Patients Hospitalized for Heart Failure: The PACT-HF Randomized Clinical Trial
Abstract
Importance: Health care services that support the hospital-to-home transition can improve outcomes in patients with heart failure (HF).
Objective: To test the effectiveness of the Patient-Centered Care Transitions in HF transitional care model in patients hospitalized for HF.
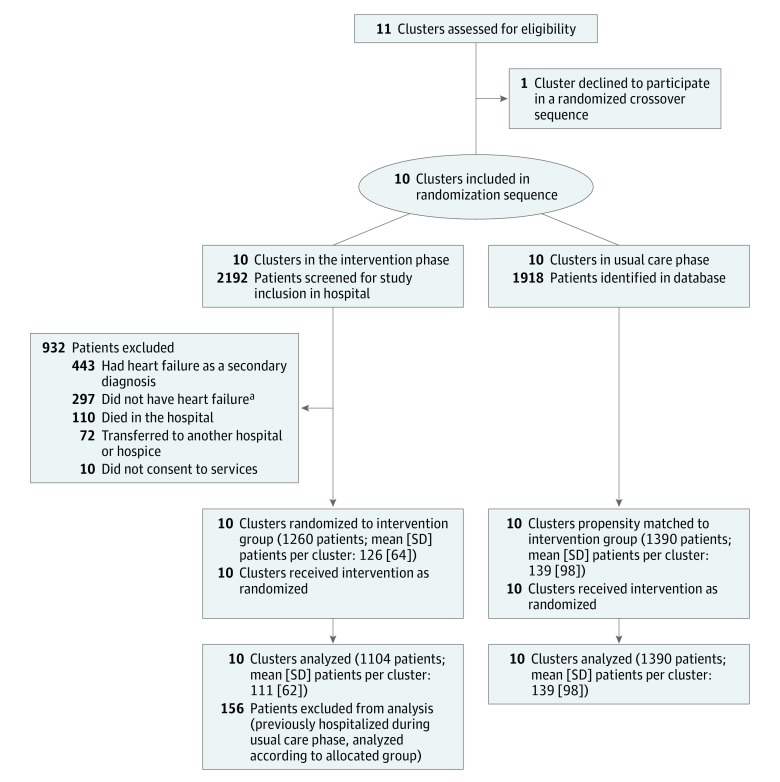
Design, setting, and participants: Stepped-wedge cluster randomized trial of 2494 adults hospitalized for HF across 10 hospitals in Ontario, Canada, from February 2015 to March 2016, with follow-up until November 2016.
Interventions: Hospitals were randomized to receive the intervention (n = 1104 patients), in which nurse-led self-care education, a structured hospital discharge summary, a family physician follow-up appointment less than 1 week after discharge, and, for high-risk patients, structured nurse homevisits and heart function clinic care were provided to patients, or usual care (n = 1390 patients), in which transitional care was left to the discretion of clinicians.
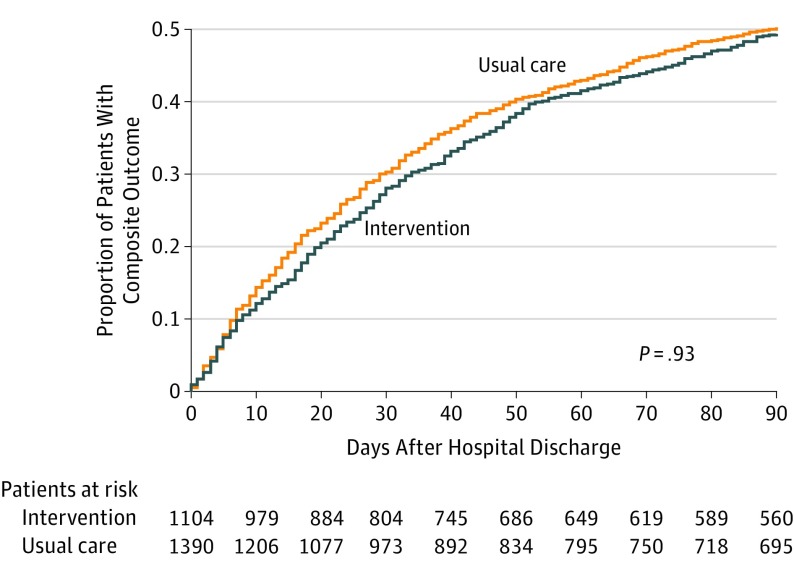
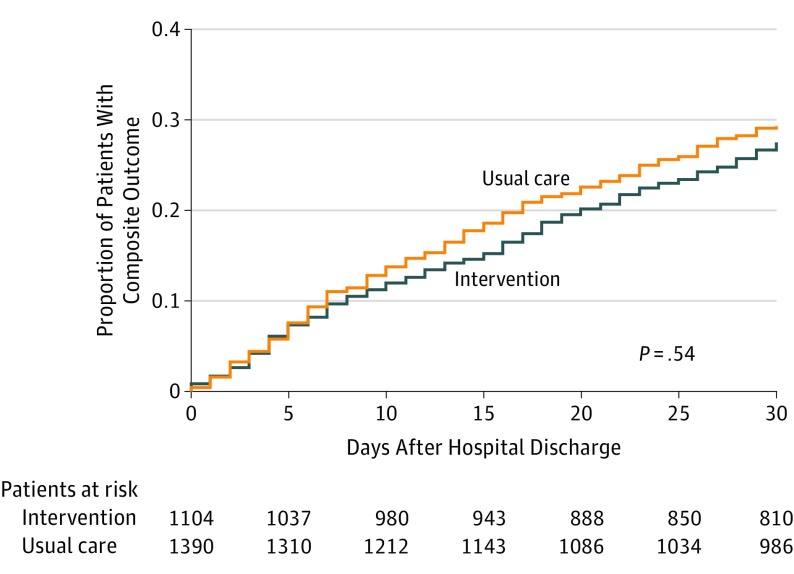
Main outcomes and measures: Primary outcomes were hierarchically ordered as composite all-cause readmission, emergency department (ED) visit, or death at 3 months; and composite all-cause readmission or ED visit at 30 days. Secondary outcomes were B-PREPARED score for discharge preparedness (range: 0 [most prepared] to 22 [least prepared]); the 3-Item Care Transitions Measure (CTM-3) for quality of transition (range: 0 [worst transition] to 100 [best transition]); the 5-level EQ-5D version (EQ-5D-5L) for quality of life (range: 0 [dead] to 1 [full health]); and quality-adjusted life-years (QALY; range: 0 [dead] to 0.5 [full health at 6 months]).
Results: Among eligible patients, all 2494 (mean age, 77.7 years; 1258 [50.4%] women) completed the trial. There was no significant difference between the intervention and usual care groups in the first primary composite outcome (545 [49.4%] vs 698 [50.2%] events, respectively; hazard ratio [HR], 0.99 [95% CI, 0.83-1.19]) or in the second primary composite outcome (304 [27.5%] vs 408 [29.3%] events, respectively; HR, 0.93 [95% CI, 0.73-1.18]). There were significant differences between the intervention and usual care groups in the secondary outcomes of mean B-PREPARED score at 6 weeks (16.6 vs 13.9; difference, 2.65 [95% CI, 1.37-3.92]; P < .001); mean CTM-3 score at 6 weeks (76.5 vs 70.3; difference, 6.16 [95% CI, 0.90-11.43]; P = .02); and mean EQ-5D-5L score at 6 weeks (0.7 vs 0.7; difference, 0.06 [95% CI, 0.01 to 0.11]; P = .02) and 6 months (0.7 vs 0.6; difference, 0.06 [95% CI, 0.01-0.12]; P = .02). There was no significant difference in mean QALY between groups at 6 months (0.3 vs 0.3; difference, 0.00 [95% CI, -0.02 to 0.02]; P = .98).
Conclusions and relevance: Among patients with HF in Ontario, Canada, implementation of a patient-centered transitional care model compared with usual care did not improve a composite of clinical outcomes. Whether this type of intervention could be effective in other health care systems or locations would require further research.
Trial registration: ClinicalTrials.gov Identifier: NCT02112227.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
