

Identifying dementia outcomes in UK Biobank: a validation study of primary care, hospital admissions and mortality data
- PMID: 30806901
- PMCID: PMC6497624
- DOI: 10.1007/s10654-019-00499-1
Identifying dementia outcomes in UK Biobank: a validation study of primary care, hospital admissions and mortality data
Abstract
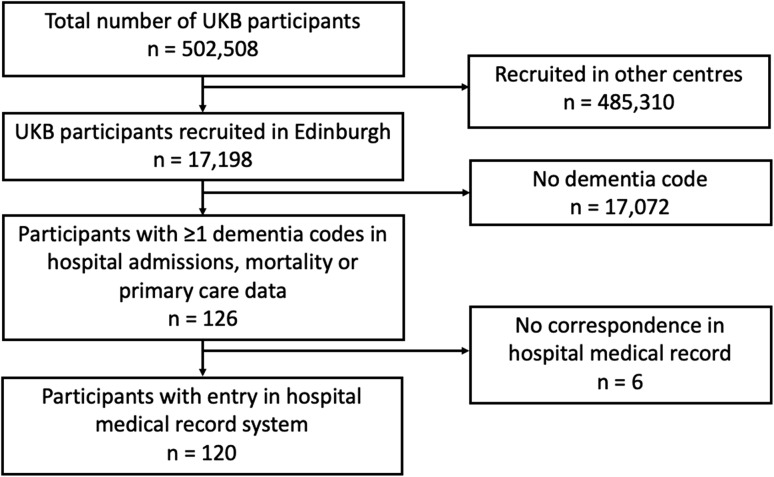
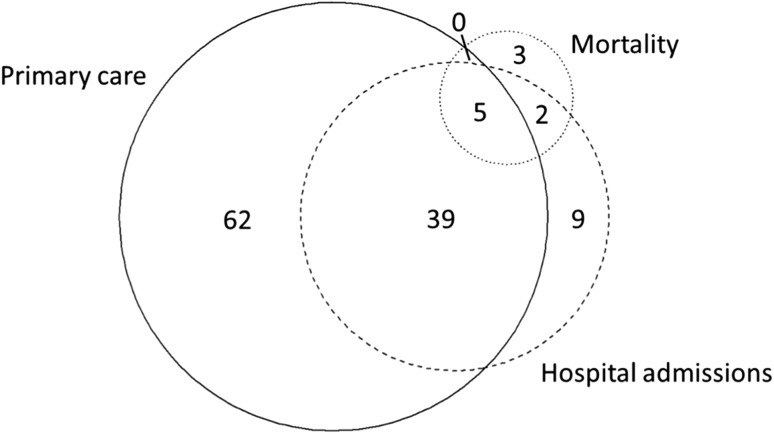
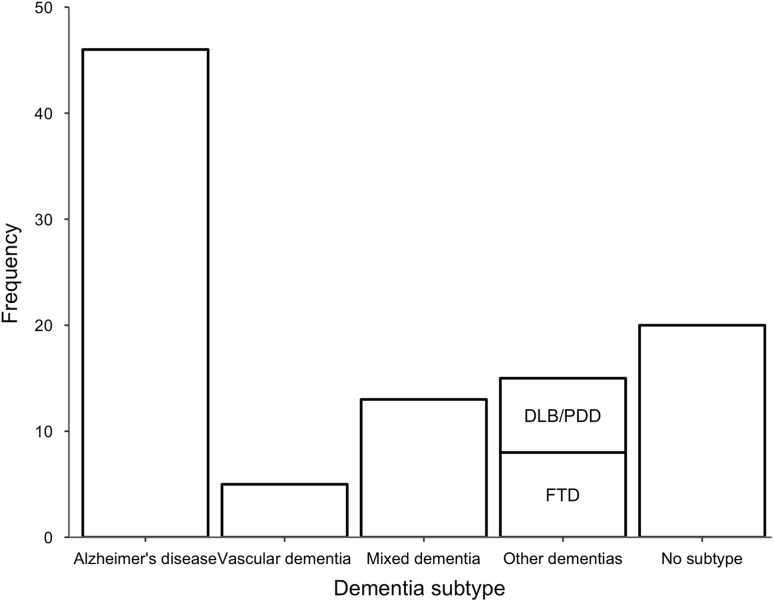
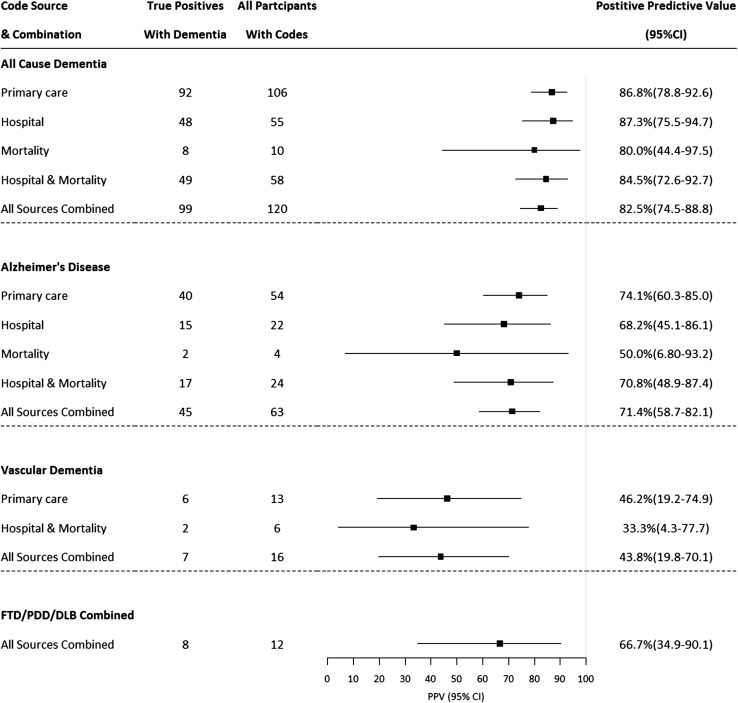
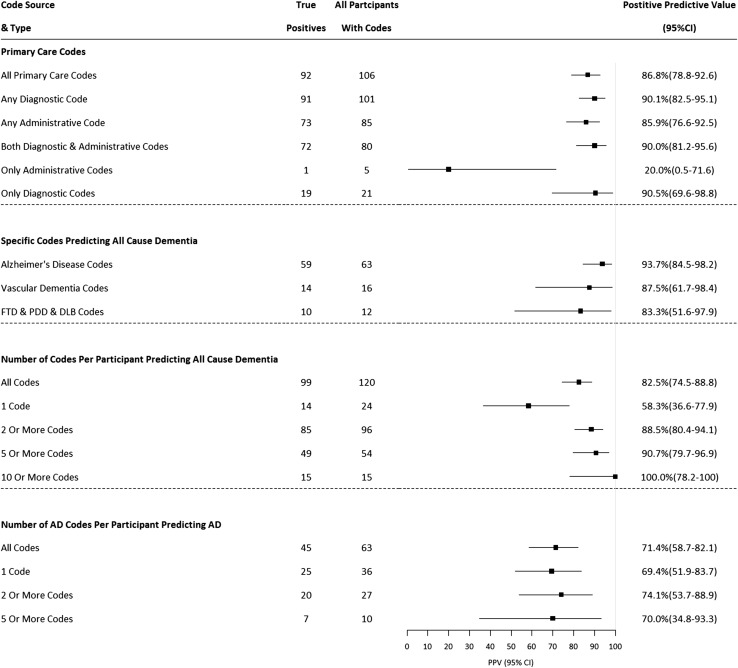
Prospective, population-based studies that recruit participants in mid-life are valuable resources for dementia research. Follow-up in these studies is often through linkage to routinely-collected healthcare datasets. We investigated the accuracy of these datasets for dementia case ascertainment in a validation study using data from UK Biobank-an open access, population-based study of > 500,000 adults aged 40-69 years at recruitment in 2006-2010. From 17,198 UK Biobank participants recruited in Edinburgh, we identified those with ≥ 1 dementia code in their linked primary care, hospital admissions or mortality data and compared their coded diagnoses to clinical expert adjudication of their full-text medical record. We calculated the positive predictive value (PPV, the proportion of cases identified that were true positives) for all-cause dementia, Alzheimer's disease and vascular dementia for each dataset alone and in combination, and explored algorithmic code combinations to improve PPV. Among 120 participants, PPVs for all-cause dementia were 86.8%, 87.3% and 80.0% for primary care, hospital admissions and mortality data respectively and 82.5% across all datasets. We identified three algorithms that balanced a high PPV with reasonable case ascertainment. For Alzheimer's disease, PPVs were 74.1% for primary care, 68.2% for hospital admissions, 50.0% for mortality data and 71.4% in combination. PPV for vascular dementia was 43.8% across all sources. UK routinely-collected healthcare data can be used to identify all-cause dementia in prospective studies. PPVs for Alzheimer's disease and vascular dementia are lower. Further research is required to explore the geographic generalisability of these findings.
Keywords: Alzheimer disease; Cohort studies; Data accuracy; Dementia; Predictive value of tests; Validation studies.
Conflict of interest statement
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
As part of the UK Biobank recruitment process, informed consent was obtained from all individual participants included in the study.
Figures
References
-
- Prince M, Wimo A, Guerchet M, Ali G-C, Wu Y-T, Prina M. World Alzheimer Report 2015: the global impact of dementia. 2015 Aug.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
