

Benefit of Early Statin Initiation within 48 Hours after Admission in Statin-Naïve Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention
- PMID: 30808084
- PMCID: PMC6511534
- DOI: 10.4070/kcj.2018.0341
Benefit of Early Statin Initiation within 48 Hours after Admission in Statin-Naïve Patients with Acute Myocardial Infarction Undergoing Percutaneous Coronary Intervention
Abstract
Background and objectives: Although current guidelines recommend early initiation of statin in patients with acute myocardial infarction (AMI), there is no consensus for optimal timing of statin initiation.
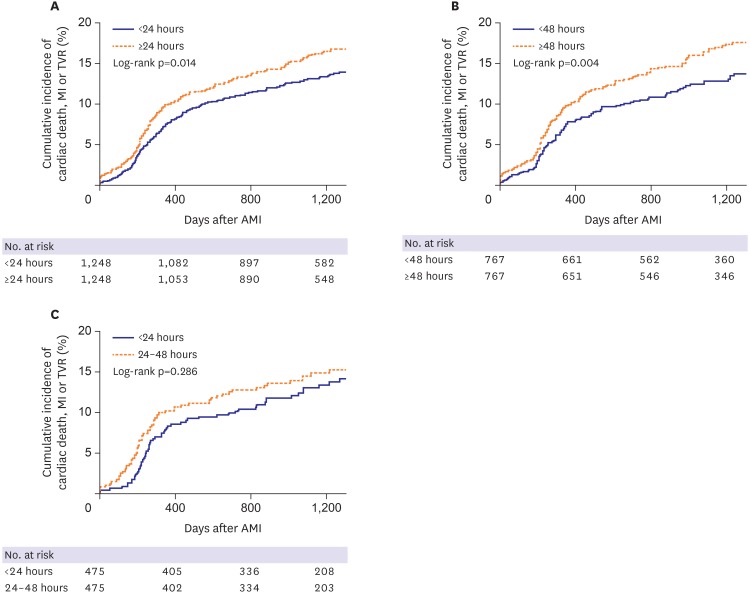
Methods: A total of 3,921 statin-naïve patients undergoing percutaneous coronary intervention were analyzed, and divided into 3 groups according to statin initiation time: group 1 (statin initiation <24 hours after admission), group 2 (24-48 hours) and group 3 (≥48 hours). We also made 3 stratified models to reduce bias: model 1 (<24 hours vs. ≥24 hours), model 2 (<48 hours vs. ≥48 hours) and model 3 (<24 hours vs. 24-48 hours). The endpoint was major adverse cardiac events (MACE; composite of cardiac death, myocardial infarction and target-vessel revascularization) during median 3.8 years.
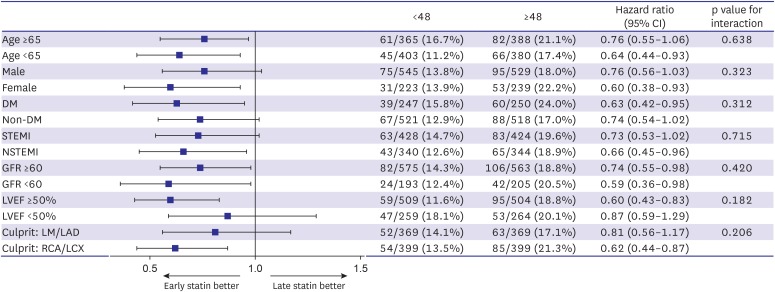
Results: During follow-up, incidence of MACE was lower in early statin group in both model 1 (14.3% vs. 18.4%, hazard ratio [HR], 0.77; 95% confidence interval [CI], 0.66-0.91; p=0.002) and model 2 (14.6% vs. 19.7%, HR, 0.81; 95% CI, 0.67-0.97; p=0.022). After propensity-score matching, results remained unaltered. Statin initiation <24 hours reduced MACE compared to statin initiation ≥24 hours in model 1. Statin initiation <48 hours also reduced MACE compared to statin initiation later in model 2. However, there was no difference in incidence of MACE between statin initiation <24 hours and 24-48 hours) in model 3.
Conclusions: Early statin therapy within 48 hours after admission in statin-naïve patients with AMI reduced long-term clinical outcomes compared with statin initiation later.
Trial registration: ClinicalTrials.gov Identifier: NCT02385682.
Keywords: Hydroxymethylglutaryl-CoA reductase inhibitors; Myocardial infarction; Percutaneous coronary intervention.
Copyright © 2019. The Korean Society of Cardiology.
Conflict of interest statement
The authors have no financial conflicts of interest.
Figures
References
-
- Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. - PubMed
-
- Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: task force for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2016;37:267–315. - PubMed
-
- O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;61:e78–140. - PubMed
-
- Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC guideline for the management of patients with non-ST-elevation acute coronary syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;64:e139–228. - PubMed
-
- Kim MC, Ahn Y, Cho KH, et al. Early statin therapy within 48 hours decreased one-year major adverse cardiac events in patients with acute myocardial infarction. Int Heart J. 2011;52:1–6. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
