

Venous Thromboembolism Prophylaxis and Risk for Acutely Medically Ill Patients Stratified by Different Ages and Renal Disease Status
- PMID: 30808218
- PMCID: PMC6714996
- DOI: 10.1177/1076029618823287
Venous Thromboembolism Prophylaxis and Risk for Acutely Medically Ill Patients Stratified by Different Ages and Renal Disease Status
Abstract
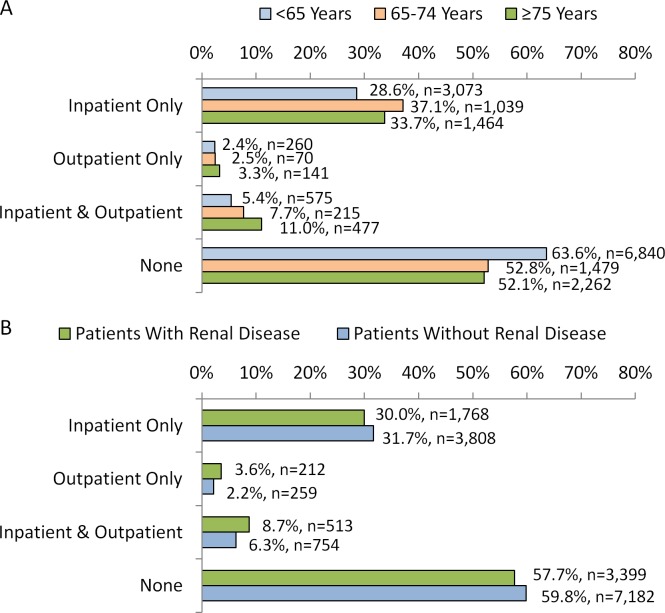
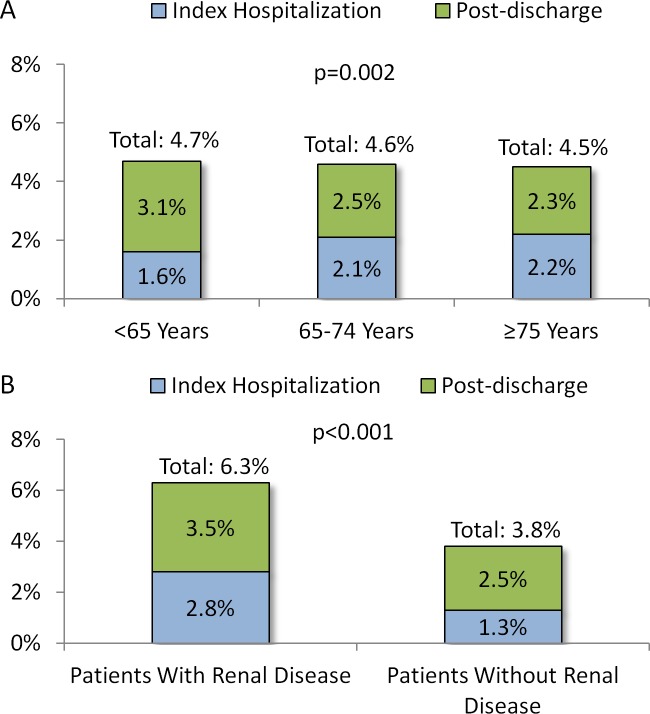
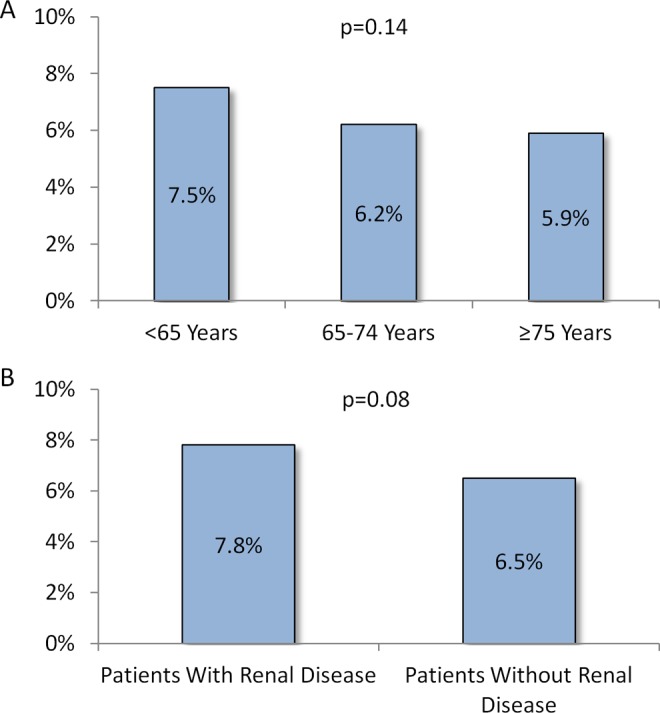
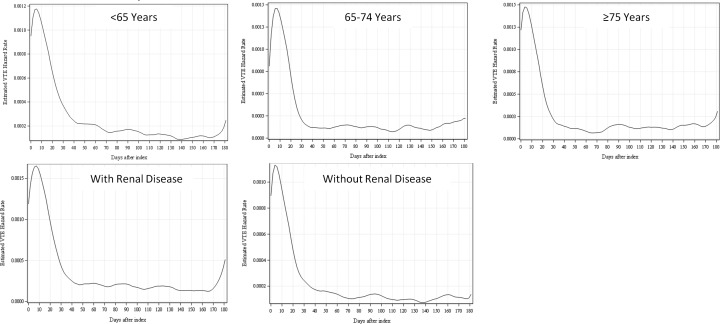
The objectives of this study were to examine venous thromboembolism (VTE) prophylaxis patterns and risk for VTE events during hospitalization and in the outpatient continuum of care among patients hospitalized for acute illnesses in the United States with stratification by different age groups and renal disease status. Acutely ill hospitalized patients were identified from the MarketScan databases (January 1, 2012-June 30, 2015) and grouped by age (<65, 65-74, ≥75 years old) and whether or not they had a baseline diagnosis of renal disease, separately. Of acutely ill hospitalized patients, 60.1% (n = 10 748) were <65 years old, 15.7% (n = 2803) were 65 to 74 years old, and 24.3% (n = 4344) were ≥75 years old; 32.9% (n = 5892) had baseline renal disease. Among the study cohorts, the majority of patients received no VTE prophylaxis regardless of age or baseline renal status (52.1%-63.6%). Rates of VTE during hospitalization and in the 6 months postdischarge were 4.7%, 4.6%, and 4.5% for patients <65, 65 to 74, and ≥75 years old, respectively, and 6.3% and 3.8% for patients with and without baseline renal disease. The risk for VTE was elevated for 30 to 40 days after index admission regardless of age and renal disease status.
Keywords: VTE prophylaxis; acute medical illness; elderly; hospitalized patients; inpatient and outpatient continuum of care; renal disease; venous thromboembolism.
Conflict of interest statement
Figures
Similar articles
-
Venous Thromboembolism Prophylaxis and Risk in the Inpatient and Outpatient Continuum of Care Among Hospitalized Acutely Ill Patients in the US: A Retrospective Analysis.Adv Ther. 2019 Jan;36(1):59-71. doi: 10.1007/s12325-018-0846-2. Epub 2018 Dec 12. Adv Ther. 2019. PMID: 30543037
-
Pharmacological Prophylaxis for Venous Thromboembolism Among Hospitalized Patients With Acute Medical Illness: An Electronic Medical Records Study.Am J Ther. 2016 Mar-Apr;23(2):e328-35. doi: 10.1097/01.mjt.0000433945.70911.7c. Am J Ther. 2016. PMID: 26720163
-
Extended Venous Thromboembolism Prophylaxis in Medically Ill Patients.Pharmacotherapy. 2018 Jun;38(6):597-609. doi: 10.1002/phar.2102. Epub 2018 Apr 25. Pharmacotherapy. 2018. PMID: 29543384 Review.
-
Venous thromboembolism prophylaxis and clinical consequences in medically ill patients.Am J Ther. 2013 Mar-Apr;20(2):132-42. doi: 10.1097/MJT.0b013e31826910dd. Am J Ther. 2013. PMID: 23466619
-
Betrixaban: a direct oral inhibitor of activated factor X for the prophylaxis of venous thromboembolism in patients hospitalized for acute medical illness.Drugs Today (Barc). 2017 Aug;53(8):423-434. doi: 10.1358/dot.2017.53.8.2681448. Drugs Today (Barc). 2017. PMID: 29119147 Review.
Cited by
-
Pulmonary Embolism in Post-CoviD-19 Patients, a Literature Review: Red Flag for Increased Awareness?SN Compr Clin Med. 2022;4(1):190. doi: 10.1007/s42399-022-01273-3. Epub 2022 Aug 19. SN Compr Clin Med. 2022. PMID: 35999860 Free PMC article. Review.
-
Diagnostic value of systematic compression ultrasonography for the detection of unrecognized venous thromboembolism in patients admitted to an internal medicine ward for dyspnea.Intern Emerg Med. 2025 Jan;20(1):181-187. doi: 10.1007/s11739-024-03773-7. Epub 2024 Nov 6. Intern Emerg Med. 2025. PMID: 39503966 Free PMC article.
-
Postdischarge thrombosis and hemorrhage in patients with COVID-19.Blood. 2020 Sep 10;136(11):1342-1346. doi: 10.1182/blood.2020007938. Blood. 2020. PMID: 32766883 Free PMC article.
-
Estimation of Acutely Ill Medical Patients at Venous Thromboembolism Risk Eligible for Extended Thromboprophylaxis Using APEX Criteria in US Hospitals.Clin Appl Thromb Hemost. 2019 Jan-Dec;25:1076029619880008. doi: 10.1177/1076029619880008. Clin Appl Thromb Hemost. 2019. PMID: 31588785 Free PMC article.
-
Post-discharge Thromboembolic Events in COVID-19 Patients: A Review on the Necessity for Prophylaxis.Clin Appl Thromb Hemost. 2023 Jan-Dec;29:10760296221148477. doi: 10.1177/10760296221148477. Clin Appl Thromb Hemost. 2023. PMID: 36596272 Free PMC article. Review.
References
-
- Mahan CE, Borrego ME, Woersching AL, et al. Venous thromboembolism: Annualised United States models for total, hospital-acquired and preventable costs utilising long-term attack rates. Thromb Haemost. 2012;108(2):291–302. - PubMed
-
- Alikhan R, Cohen AT, Combe S, et al. Risk factors for venous thromboembolism in hospitalized patients with acute medical illness: analysis of the MEDENOX Study. Arch Intern Med. 2004;164(9):963–968. - PubMed
