

Semi-automated computed tomography Volumetry can predict hemihepatectomy specimens' volumes in patients with hepatic malignancy
- PMID: 30808320
- PMCID: PMC6390596
- DOI: 10.1186/s12880-019-0309-5
Semi-automated computed tomography Volumetry can predict hemihepatectomy specimens' volumes in patients with hepatic malignancy
Abstract
Background: One of the major causes of perioperative mortality of patients undergoing major hepatic resections is post-hepatectomy liver failure (PHLF). For preoperative appraisal of the risk of PHLF it is important to accurately predict resectate volume and future liver remnant volume (FLRV). The objective of our study is to prospectively evaluate the accuracy of hemihepatectomy resectate volumes that are determined by computed tomography volumetry (CTV) when compared with intraoperatively measured volumes and weights as gold standard in patients undergoing hemihepatectomy.
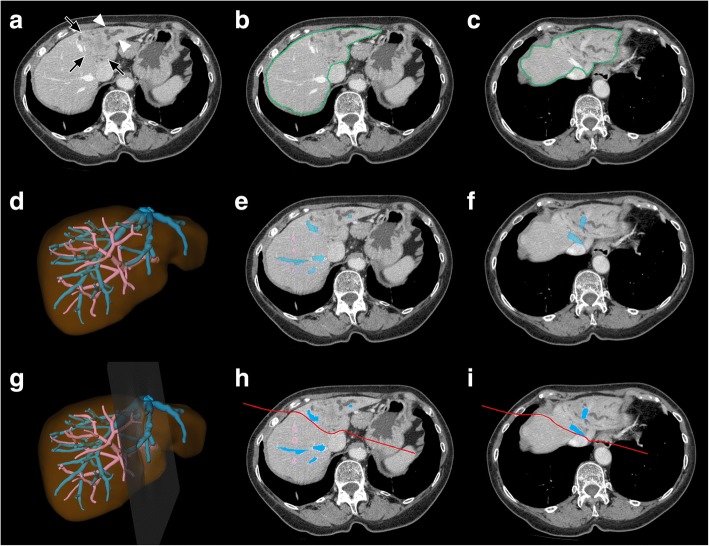
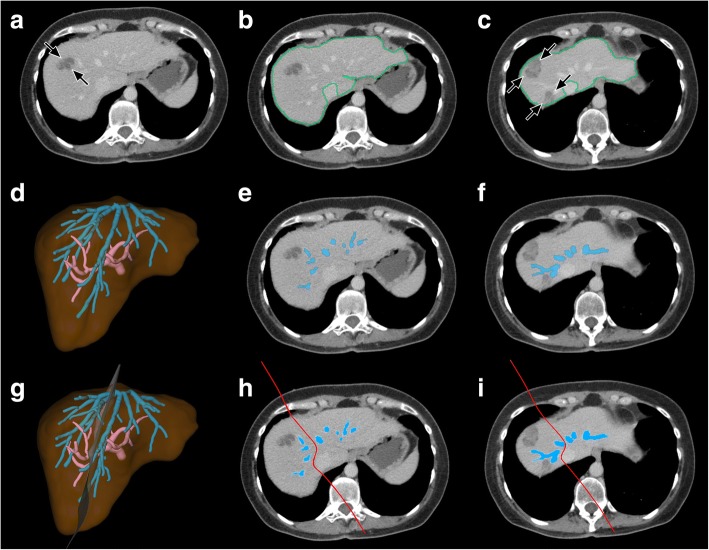
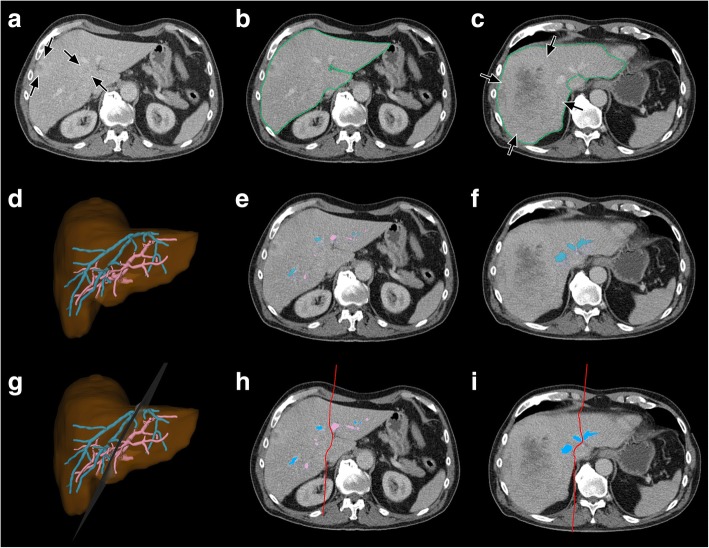
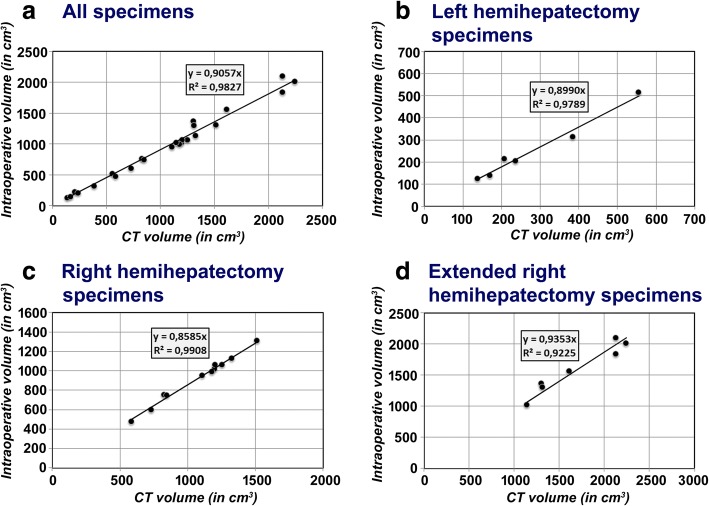
Methods: Twenty four patients (13 women, 11 men) scheduled for hemihepatectomy due to histologically proven primary or secondary hepatic malignancies were included in our study. CTV was performed using a semi-automated module (S, hereinafter) (syngo.CT Liver Analysis VA30, Siemens Healthcare, Germany). Conversion factors between CT volumes on the one side and intraoperative volumes and weights on the other side were calculated using the method of least squares. Absolute and relative disagreements between CT volumes and intraoperative volumes were determined.
Results: A conversion factor of c = 0.906 most precisely predicted intraoperative volumes of exsanguinated hemihepatectomy specimens from CT volumes in all patients with mean absolute and relative disagreements between CT volumes and intraoperative volumes of 57 ml and 6.3%. The use of operation-specific conversion factors yielded even better results.
Conclusions: CTV performed with S accurately predicts intraoperative volumes of hemihepatectomy specimens when applying conversion factors which compensate for exsanguination. This allows to precisely estimate the FLRV and thus minimize the risk of PHLF in patients undergoing major hepatic resections.
Keywords: Computed tomography volumetry; Hemihepatectomy; Hepatic malignancy.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (Ethikkommission der Medizinischen Fakultät Heidelberg, Heidelberg, Germany, approval number: S-192/2013). All procedures performed were in accordance with the declaration of Helsinki. Written informed consent was obtained from all individual participants included in the study.
Consent for publication
Not applicable.
Competing interests
This study was supported financially by Siemens Healthcare, Germany.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Schindl MJ, Redhead DN, Fearon KCH, Garden OJ, Wigmore SJ. Edinburgh liver surgery and transplantation experimental research group (eLISTER). The value of residual liver volume as a predictor of hepatic dysfunction and infection after major liver resection. Gut. 2005;54:289–296. doi: 10.1136/gut.2004.046524. - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
