

The effect of hyperoxia on mortality in critically ill patients: a systematic review and meta analysis
- PMID: 30808337
- PMCID: PMC6390560
- DOI: 10.1186/s12890-019-0810-1
The effect of hyperoxia on mortality in critically ill patients: a systematic review and meta analysis
Abstract
Background: Studies investigating the role of hyperoxia in critically ill patients have reported conflicting results. We did this analysis to reveal the effect of hyperoxia in the patients admitted to the intensive care unit (ICU).
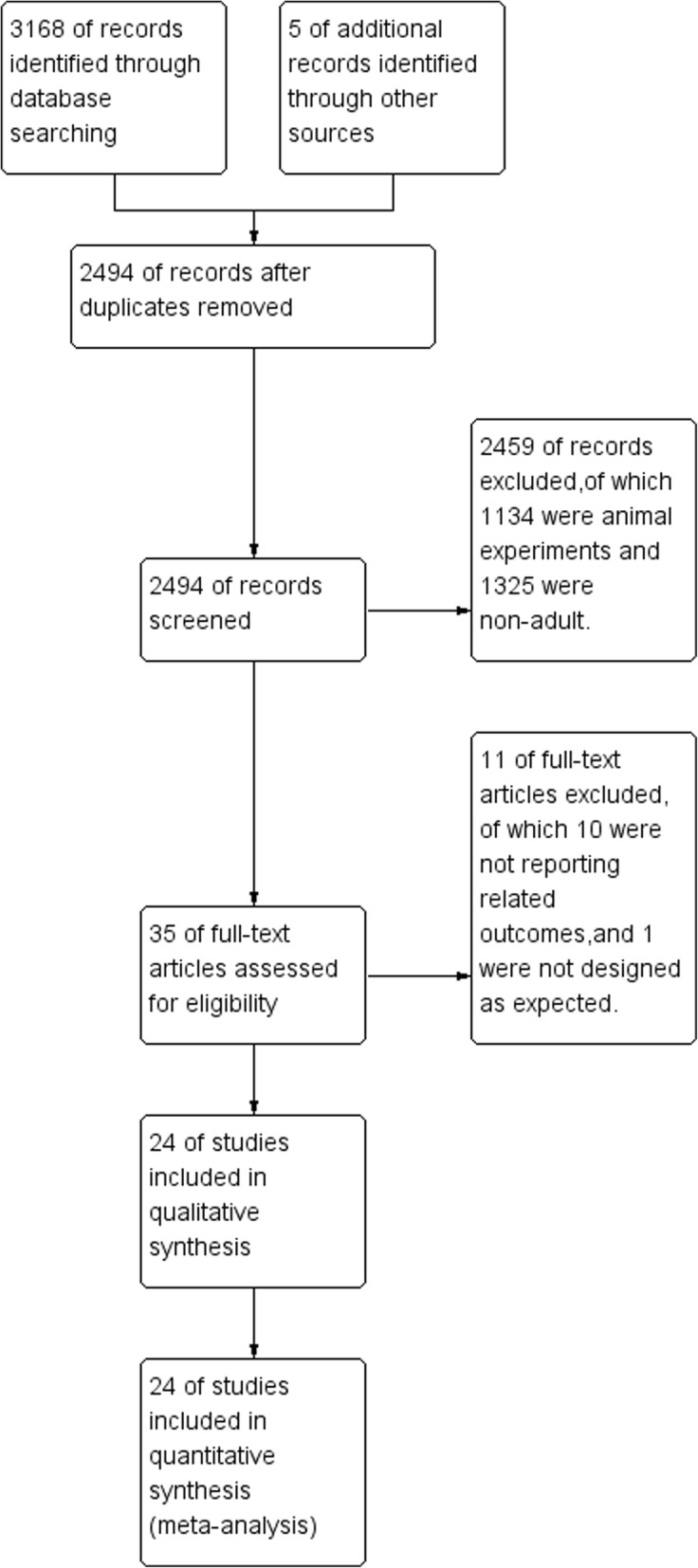
Methods: Electronic databases were searched for all the studies exploring the role of hyperoxia in adult patients admitted to ICU. The primary outcome was mortality. Random-effect model was used for quantitative synthesis of the adjusted odds ratio (aOR).
Results: We identified 24 trials in our final analysis. Statistical heterogeneity was found between hyperoxia and normoxia groups in patients with mechanical ventilation (I2 = 92%, P < 0.01), cardiac arrest(I2 = 63%, P = 0.01), traumatic brain injury (I2 = 85%, P < 0.01) and post cardiac surgery (I2 = 80%, P = 0.03). Compared with normoxia, hyperoxia was associated with higher mortality in overall patients (OR 1.22, 95% CI 1.12~1.33), as well as in the subgroups of cardiac arrest (OR 1.30, 95% CI 1.08~1.57) and extracorporeal life support (ELS) (OR 1.44, 95% CI 1.03~2.02).
Conclusions: Hyperoxia would lead to higher mortality in critically ill patients especially in the patients with cardiac arrest and ELS.
Keywords: Hyperoxia; Meta-analysis; Mortality.
Conflict of interest statement
Ethics approval and consent to participate
Our study was approved by the Institutional Ethical Committee for Clinical and Biomedical Research of West China Hospital (Sichuan, China).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Esteban A, Anzueto A, Alía I, Gordo F, Apezteguía C, Pálizas F, Cide D, Goldwaser R, Soto L, Bugedo G, et al. How is mechanical ventilation employed in the intensive care unit? An international utilization review. Am J Respir Crit Care Med. 2000;161(5):1450–1458. - PubMed
-
- Helmerhorst HJ, Schultz MJ, van der Voort PH, Bosman RJ, Juffermans NP, de Wilde RB, van den Akker-van Marle ME, van Bodegom-Vos L, de Vries M, Eslami S, et al. Effectiveness and clinical outcomes of a two-step implementation of conservative oxygenation targets in critically ill patients: a before and after trial. Crit Care Med. 2016;44(3):554–563. - PubMed
-
- Altemeier WA, Sinclair SE. Hyperoxia in the intensive care unit: why more is not always better. Curr Opin Crit Care. 2007;13(1):73–78. - PubMed
-
- Sinclair SE, Altemeier WA, Matute-Bello G, Chi EY. Augmented lung injury due to interaction between hyperoxia and mechanical ventilation. Crit Care Med. 2004;32(12):2496–2501. - PubMed
-
- Lodato RF. Decreased O2 consumption and cardiac output during normobaric hyperoxia in conscious dogs. J Appl Physiol (1985) 1989;67(4):1551–1559. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
