

Cost of Disease Progression in Patients with Chronic Lymphocytic Leukemia, Acute Myeloid Leukemia, and Non-Hodgkin's Lymphoma
- PMID: 30808814
- PMCID: PMC6738303
- DOI: 10.1634/theoncologist.2018-0019
Cost of Disease Progression in Patients with Chronic Lymphocytic Leukemia, Acute Myeloid Leukemia, and Non-Hodgkin's Lymphoma
Abstract
Introduction: To reduce health care costs and improve care, payers and physician groups are switching to quality-based and episodic or bundled-care models. Disease progression and associated costs may affect these models, particularly if such programs do not account for differences in disease severity and progression risk within the cohort. This study estimated the incremental cost of disease progression in patients diagnosed with chronic lymphoid leukemia (CLL), acute myeloid leukemia (AML), and non-Hodgkin's lymphoma (NHL) and compared costs among patients with and without progression.
Methods: This was a retrospective study using U.S. administrative claims data from commercial and Medicare Advantage health care enrollees with evidence of CLL, AML, and NHL and systemic antineoplastic agent use from July 1, 2006 to August 31, 2014. Outcome measures included disease progression, 12-month health care costs, and 3-year cumulative predictive health care costs.
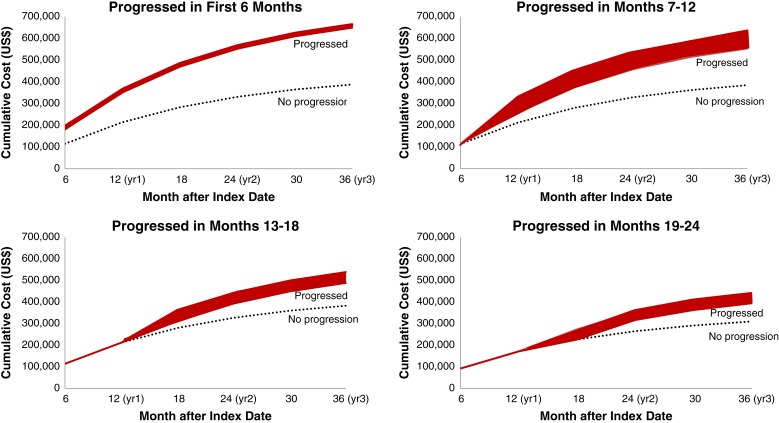
Results: Of 1,056 patients with CLL, 514 patients with AML, and 7,601 patients with NHL, 31.1% of patients with CLL, 63.8% of those with AML, and 36.9% of those with NHL had evidence of disease progression. Among patients with CLL and NHL, adjusted and unadjusted health care costs were significantly higher among progressors versus nonprogressors. Per-patient-per-month costs, accounting for variable follow-up time, were almost twice as high among progressors versus nonprogressors in patients with CLL, AML, and NHL. In each of the three cancer types, the longer disease progression was delayed, the lower the health care costs.
Conclusion: Progression of CLL, AML, and NHL was associated with higher health care costs over a 12-month period. Delaying cancer progression resulted in a substantial cost reduction in patients with all three cancer types.
Implications for practice: Data on the rates and incremental health care costs of disease progression in patients with hematologic malignancies are lacking. This study estimated the incremental costs of disease progression in patients diagnosed with chronic lymphocytic leukemia, acute myeloid leukemia, and non-Hodgkin's lymphoma and compared health care costs in patients with and without evidence of disease progression in a real-world population. The data obtained in this study will assist future studies in quantifying the cost impact of decreased progression rates and will inform payers and physician groups about setting rates for episode and bundled payment programs.
Keywords: Acute myeloid leukemia; Chronic lymphocytic leukemia; Costs; Non‐Hodgkin's lymphoma; Progression.
© AlphaMed Press 2019.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures





Similar articles
-
Cost of Disease Progression in Patients with Metastatic Breast, Lung, and Colorectal Cancer.Oncologist. 2019 Sep;24(9):1209-1218. doi: 10.1634/theoncologist.2018-0018. Epub 2019 Feb 22. Oncologist. 2019. PMID: 30796156 Free PMC article.
-
Time to Next Treatment, Health Care Resource Utilization, and Costs Associated with Ibrutinib Use Among U.S. Veterans with Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma: A Real-World Retrospective Analysis.J Manag Care Spec Pharm. 2020 Oct;26(10):1266-1275. doi: 10.18553/jmcp.2020.20095. Epub 2020 Sep 3. J Manag Care Spec Pharm. 2020. PMID: 32880204 Free PMC article.
-
Real-world comparison of health care costs of venetoclax-obinutuzumab vs Bruton's tyrosine kinase inhibitor use among US Medicare beneficiaries with chronic lymphocytic leukemia in the frontline setting.J Manag Care Spec Pharm. 2024 Oct;30(10):1106-1116. doi: 10.18553/jmcp.2024.24049. Epub 2024 Jul 24. J Manag Care Spec Pharm. 2024. PMID: 39046941 Free PMC article.
-
Bendamustine for the treatment of indolent non-Hodgkin's lymphoma and chronic lymphocytic leukemia.Am J Health Syst Pharm. 2010 May 1;67(9):713-23. doi: 10.2146/ajhp090328. Am J Health Syst Pharm. 2010. PMID: 20410545 Review.
-
Rituximab: a review of its use in non-Hodgkin's lymphoma and chronic lymphocytic leukaemia.Drugs. 2006;66(6):791-820. doi: 10.2165/00003495-200666060-00005. Drugs. 2006. PMID: 16706552 Review.
Cited by
-
Number needed to treat and associated cost analysis of zanubrutinib vs ibrutinib in chronic lymphocytic leukemia.J Manag Care Spec Pharm. 2025 May;31(5):482-490. doi: 10.18553/jmcp.2025.24330. Epub 2025 Apr 10. J Manag Care Spec Pharm. 2025. PMID: 40207898 Free PMC article.
-
Cost-effectiveness of ropeginterferon alfa-2b-njft for the treatment of polycythemia vera.J Comp Eff Res. 2023 Sep;12(9):e230066. doi: 10.57264/cer-2023-0066. Epub 2023 Aug 2. J Comp Eff Res. 2023. PMID: 37531245 Free PMC article.
-
What Does the Economic Burden of Acute Myeloid Leukemia Treatment Look Like for the Next Decade? An Analysis of Key Findings, Challenges and Recommendations.J Blood Med. 2021 May 5;12:245-255. doi: 10.2147/JBM.S279736. eCollection 2021. J Blood Med. 2021. PMID: 33981169 Free PMC article. Review.
-
Real-world outcomes associated with switching to anti-TNFs versus other biologics in Crohn's Disease patients: A retrospective analysis using German claims data.Therap Adv Gastroenterol. 2022 Nov 4;15:17562848221130554. doi: 10.1177/17562848221130554. eCollection 2022. Therap Adv Gastroenterol. 2022. PMID: 36353736 Free PMC article.
-
Based on knowledge capital value for disease cost accounting of diagnosis related groups.Front Public Health. 2024 Jun 10;12:1269704. doi: 10.3389/fpubh.2024.1269704. eCollection 2024. Front Public Health. 2024. PMID: 38915748 Free PMC article.
References
-
- American Cancer Society . Cancer Facts & Figures 2017. Atlanta, GA: American Cancer Society; 2017. Available at https://www.cancer.org/content/dam/cancer‐org/research/cancer‐facts‐and‐.... Accessed May 10, 2017.
-
- Newcomer LN. Innovative payment models and measurement for cancer therapy. J Oncol Pract 2014;10:187–189. - PubMed
-
- Newcomer LN, Gould B, Page RD et al. Changing physician incentives for affordable, quality cancer care: Results of an episode payment model. J Oncol Pract 2014;10:322–326. - PubMed
-
- American Society of Clinical Oncology . Patient‐Centered Oncology Payment. Alexandria, VA: American Society of Clinical Oncology; 2015. Available at http://www.chqpr.org/downloads/ASCO_Patient‐centered_Oncology_Payment.pdf. Accessed May 10, 2017.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
