

Malignant Middle Cerebral Artery Infarction Due to Hyponatremia Following Traumatic Brain Injury: A Case Report
- PMID: 30808857
- PMCID: PMC6402275
- DOI: 10.12659/AJCR.913872
Malignant Middle Cerebral Artery Infarction Due to Hyponatremia Following Traumatic Brain Injury: A Case Report
Abstract
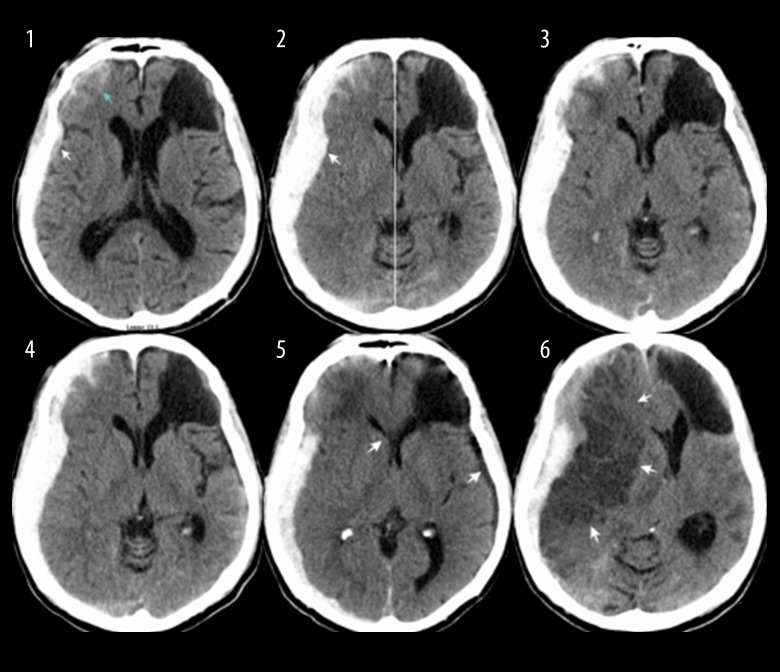
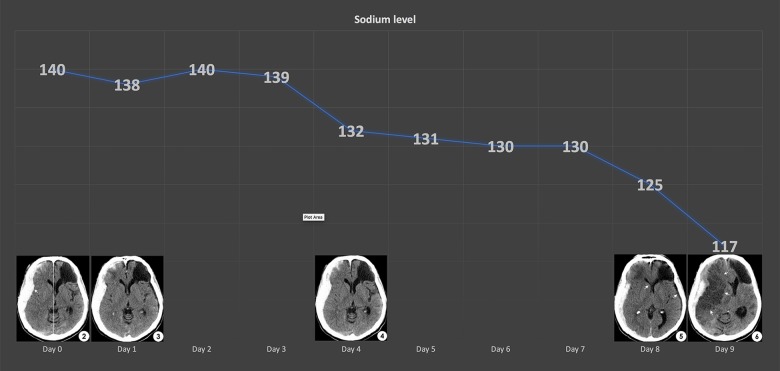
BACKGROUND Development of syndrome of inappropriate antidiuretic hormone secretion or cerebral salt wasting has been commonly noted in post-traumatic brain injury, and this condition may lead to hyponatremia resulting in cerebral edema and possible cerebral herniation. However, the predominant topographic pattern of edema from hyponatremia has not been well documented. Unlike numerous reports on hyponatremia and vasospasm following aneurysmal subarachnoid hemorrhage, the data for traumatic brain injury patient are still limited. We report on a rare patient with malignant middle cerebral artery infarction as a result of hyponatremia following traumatic brain injury. CASE REPORT A 60-year-old Native American male with significant past medical history of alcoholism, hypertension, and hemorrhagic stroke presented to the emergency department by emergency medical service after he was struck by a vehicle in a hit-and-run incident. The patient sustained multiple abrasions, and he had elevated alcohol levels. His initial Glasgow Coma Score (GCS) was 14 with a confused conversation (V4). Computer tomography (CT) of the head showed 5 mm thickness acute subdural and subarachnoid hemorrhage of right frontal, temporal, and parietal areas, with 3 mm midline shift at the level of foramen of Monro. Traumatic brain injury conservative treatment was initiated as well as alcoholic withdrawal protocols in the intensive care unit. Patient initially improved neurologically despite low sodium levels. He recouped to fully conscious, with a GCS score of 15, at 24 hours after admission. On day 9, he was found unresponsive with a head CT showed malignant right middle cerebral artery infarction, resulted in 15 mm subfalcine herniation. The patient passed away 48 hours later, as patient's family declined further intervention. CONCLUSIONS The management and prevention of post-traumatic vasospasm may be complicated even in asymptomatic and neurologically intact patients. Close neurological monitoring and prevention protocols are important in activating appropriate management.
Conflict of interest statement
None.
Figures
References
-
- Lohani S, Devkota UP. Hyponatremia in patients with traumatic brain injury: Etiology, incidence, and severity correlation. World Neurosurg. 2011;76(3):355–60. - PubMed
-
- Cole CD, Gottfried ON, Liu JK, Couldwell WT. Hyponatremia in the neurosurgical patient: Diagnosis and management. Neurosurg Focus. 2004;16(4):E9. - PubMed
-
- Fraser J, Stieg P. Hyponatremia in the neurosurgical patient: Epidemiology, pathophysiology, diagnosis, and management. Neurosurgery. 2006;59:222–29. discussion 222. - PubMed
-
- Adrogué HJ. Consequences of inadequate management of hyponatremia. Am J Nephrol. 2005;25(3):240–49. - PubMed
-
- Sturdik I, Adamcova M, Kollerova J, et al. Hyponatremia is an independent predictor of in-hospital mortality. Eur J Intern Med. 2014;25(4):379–82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
