

SMAD4 rare variants in individuals and families with thoracic aortic aneurysms and dissections
- PMID: 30809044
- PMCID: PMC6777456
- DOI: 10.1038/s41431-019-0357-x
SMAD4 rare variants in individuals and families with thoracic aortic aneurysms and dissections
Abstract
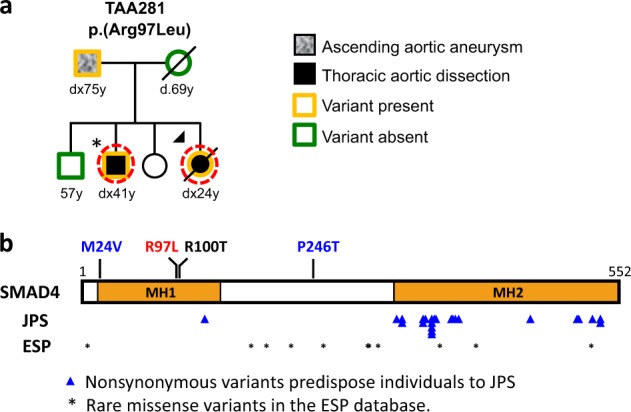
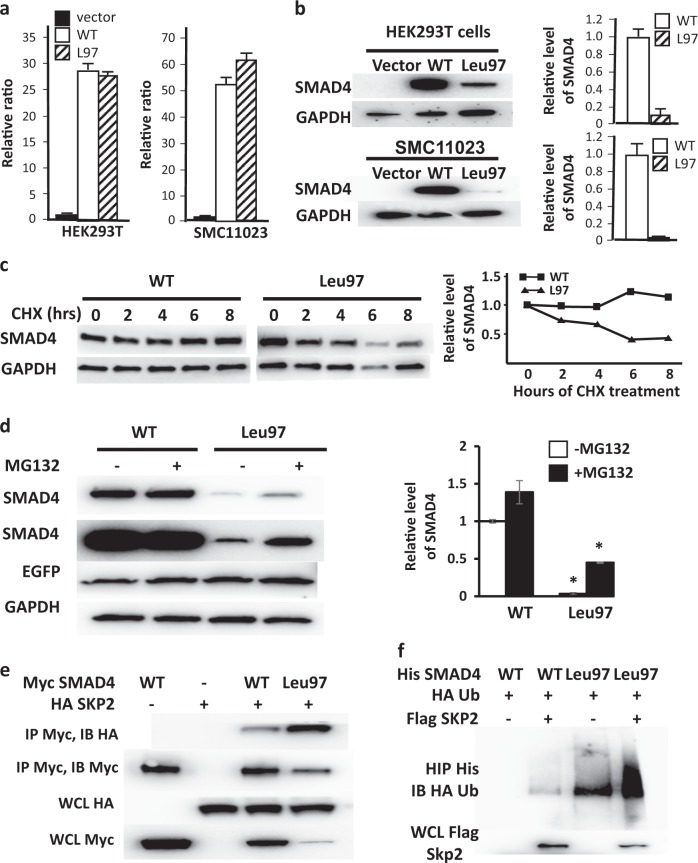
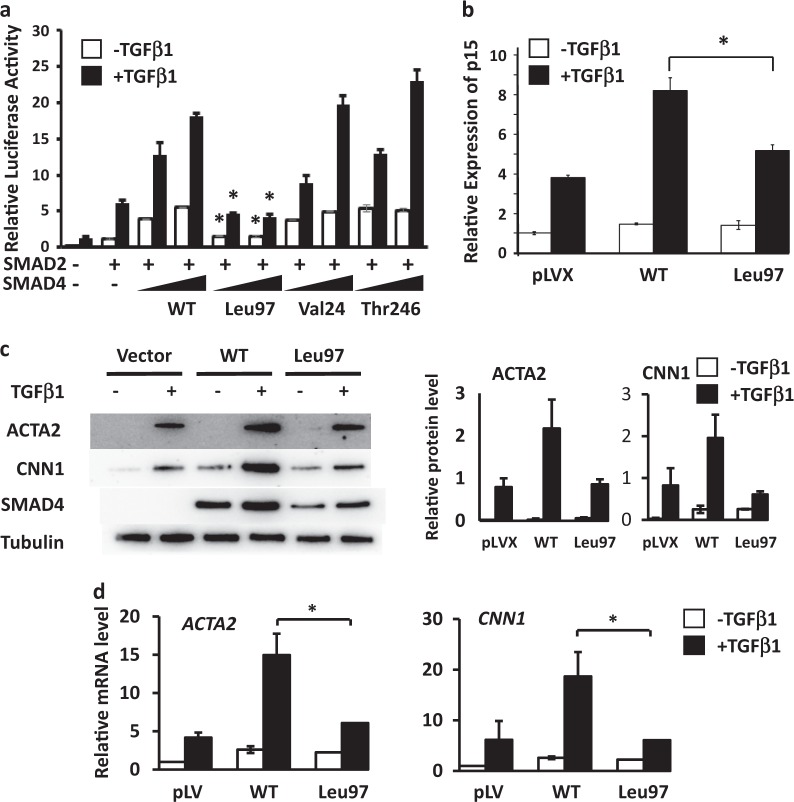
SMAD4 pathogenic variants cause juvenile polyposis (JPS) and hereditary hemorrhagic telangiectasia (HHT), and 40% of affected individuals also have thoracic aortic disease. At the same time, SMAD4 pathogenic variants have not been reported in thoracic aortic disease families without JPS-HHT. A SMAD4 heterozygous variant, c.290G>T, p.(Arg97Leu), not present in population databases and predicted to be damaging to protein function, was identified in a family with thoracic aortic disease and no evidence of HHT or JPS. Cellular studies revealed that the SMAD4 p.(Arg97Leu) alteration increased SMAD4 ubiquitination and 26S proteasome-mediated protein degradation. Smooth muscle cells (SMCs) infected with lentivirus expressing the SMAD4 p.(Arg97Leu) variant demonstrated reduced contractile protein gene expression when compared to that of wild-type SMAD4. In addition, two rare variants were identified in individuals with early age of onset of thoracic aortic dissection. These results suggest that SMAD4 rare missense variants can lead to thoracic aortic disease in individuals who do not have JPS or HHT.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Howard DP, Banerjee A, Fairhead JF, Perkins J, Silver LE, Rothwell PM. Population-based study of incidence and outcome of acute aortic dissection and premorbid risk factor control: 10-year results from the Oxford Vascular Study. Circulation. 2013;127:2031–7. doi: 10.1161/CIRCULATIONAHA.112.000483. - DOI - PMC - PubMed
-
- Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with Thoracic Aortic Disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121:e266–369. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
