

Aspiration therapy for acute embolic occlusion of the superior mesenteric artery
- PMID: 30809084
- PMCID: PMC6385017
- DOI: 10.3748/wjg.v25.i7.848
Aspiration therapy for acute embolic occlusion of the superior mesenteric artery
Abstract
Background: Embolic superior mesenteric artery (SMA) occlusion is associated with high mortality rates. Delayed treatment often leads to serious consequences, including intestinal necrosis, resection, and even patient death. Endovascular repair is being introduced, which can improve clinical symptoms and prognosis and decrease the incidence of exploratory laparotomy. Many reports have described successful endovascular revascularization of embolic SMA occlusion. However, most of those reports are case reports, and there are few reports on Chinese patients. In this paper, we describe the technical and clinical outcomes of aspiration therapy using a guiding catheter and long sheath technique which facilitates the endovascular repair procedure.
Aim: To evaluate the complications, feasibility, effectiveness, and safety of endovascular treatment for the acute embolic occlusion of the SMA.
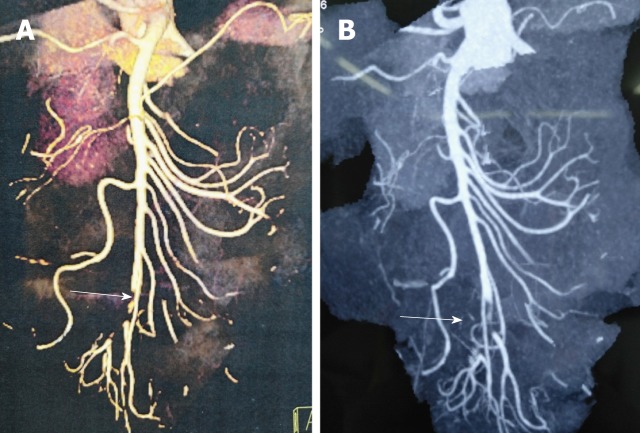
Methods: This retrospective study reviewed eight patients (six males and two females) from August 2013 to October 2018 at Xuanwu Hospital, Capital Medical University. The patients presented with acute embolic occlusion of the SMA on admission and were initially diagnosed by computed tomography angiography (CTA). The patients who underwent endovascular treatment with a guiding catheter had no obvious evidence of bowel infarct. No intestinal necrosis was identified by gastrointestinal surgeons through peritoneal puncture or CTA. The complications, feasibility, effectiveness, safety, and mortality were assessed.
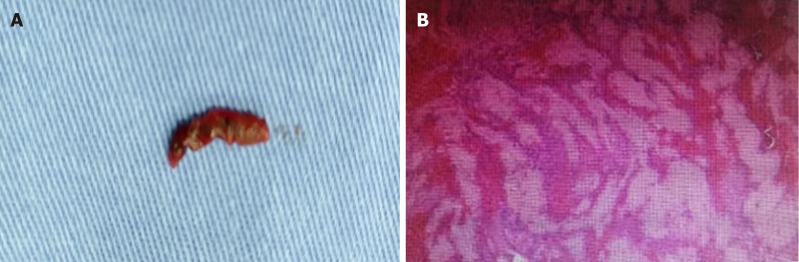
Results: Six (75%) patients were male, and the mean patient age was 70.00 ± 8.43 years (range, 60-84 years). The acute embolic occlusion of the SMA was initially diagnosed by CTA. All patients had undertaken anticoagulation primarily, and percutaneous aspiration using a guiding catheter was then undertaken because the emboli had large amounts of thrombus residue. No death occurred among the patients. Complete patency of the suffering artery trunk was achieved in six patients, and defect filling was accomplished in two patients. The in-hospital mortality was 0%. The overall 12-mo survival rate was 100%. All patients survived, and two of the eight patients had complications (the clot broke off during aspiration).
Conclusion: Aspiration therapy is feasible, safe, and beneficial for acute embolic SMA occlusion. Aspiration therapy has many benefits for reducing patients' death, resolving thrombi, and improving symptoms.
Keywords: Acute embolic occlusion; Aspiration embolectomy; Endovascular repair; Superior mesenteric artery; Transcatheter thrombolysis.
Conflict of interest statement
Conflict-of-interest statement: All authors declare no conflicts of interest related to this article.
Figures

References
-
- Björck M, Acosta S, Lindberg F, Troëng T, Bergqvist D. Revascularization of the superior mesenteric artery after acute thromboembolic occlusion. Br J Surg. 2002;89:923–927. - PubMed
-
- Gupta PK, Natarajan B, Gupta H, Fang X, Fitzgibbons RJ., Jr Morbidity and mortality after bowel resection for acute mesenteric ischemia. Surgery. 2011;150:779–787. - PubMed
-
- Schoots IG, Levi MM, Reekers JA, Lameris JS, van Gulik TM. Thrombolytic therapy for acute superior mesenteric artery occlusion. J Vasc Interv Radiol. 2005;16:317–329. - PubMed
-
- Ryer EJ, Kalra M, Oderich GS, Duncan AA, Gloviczki P, Cha S, Bower TC. Revascularization for acute mesenteric ischemia. J Vasc Surg. 2012;55:1682–1689. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
