

Increased Regulatory T-Cell Activity and Enhanced T-Cell Homeostatic Signaling in Slow Progressing HIV-infected Children
- PMID: 30809229
- PMCID: PMC6379343
- DOI: 10.3389/fimmu.2019.00213
Increased Regulatory T-Cell Activity and Enhanced T-Cell Homeostatic Signaling in Slow Progressing HIV-infected Children
Abstract
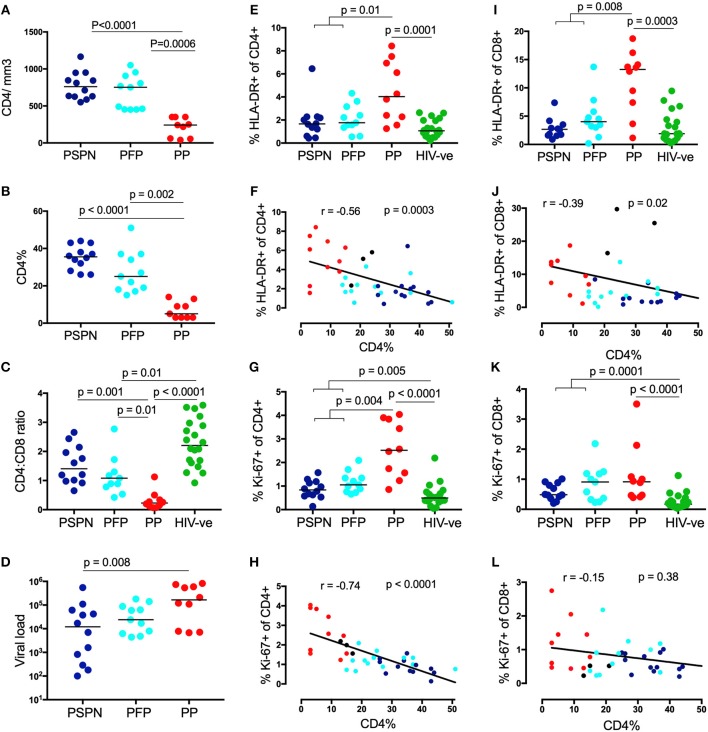
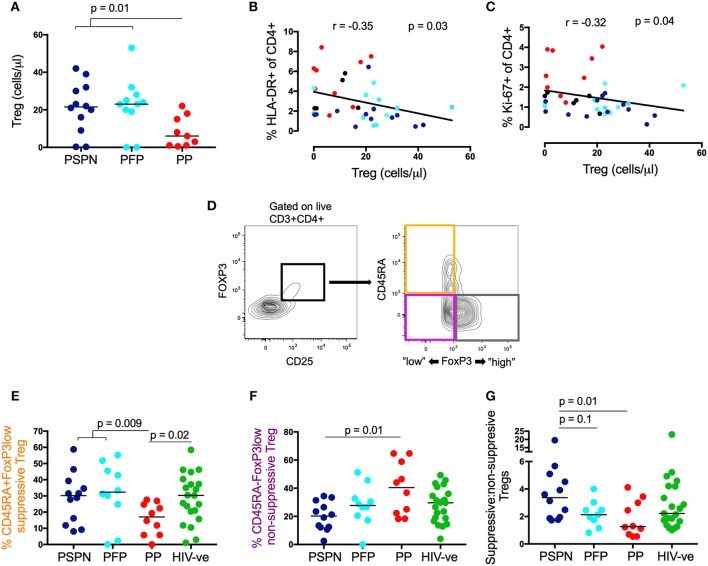
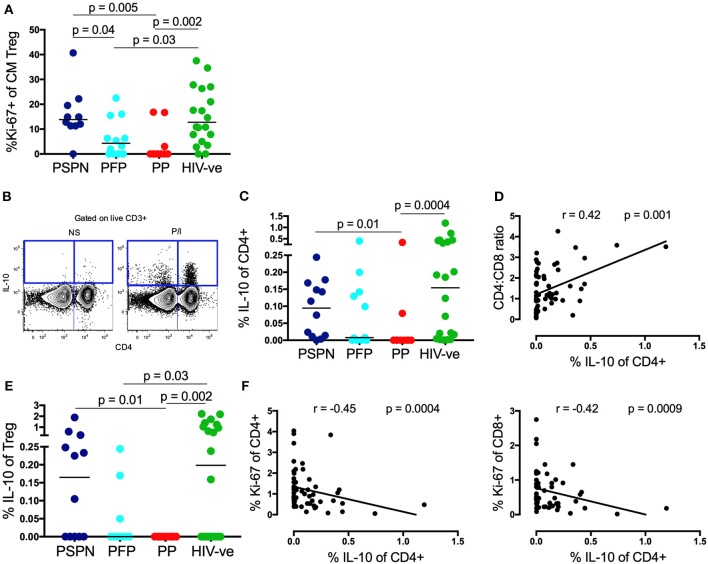
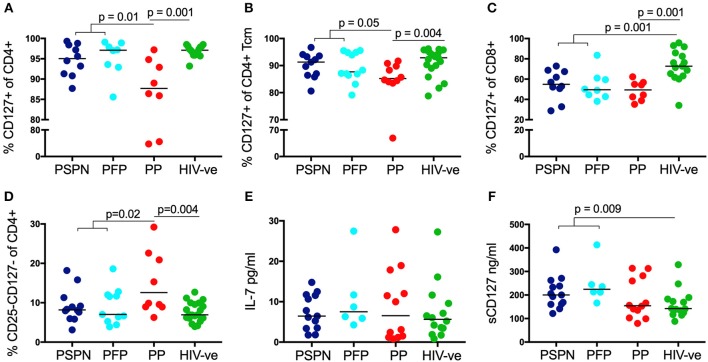
Pediatric slow progressors (PSP) are rare ART-naïve, HIV-infected children who maintain high CD4 T-cell counts and low immune activation despite persistently high viral loads. Using a well-defined cohort of PSP, we investigated the role of regulatory T-cells (TREG) and of IL-7 homeostatic signaling in maintaining normal-for-age CD4 counts in these individuals. Compared to children with progressive disease, PSP had greater absolute numbers of TREG, skewed toward functionally suppressive phenotypes. As with immune activation, overall T-cell proliferation was lower in PSP, but was uniquely higher in central memory TREG (CM TREG), indicating active engagement of this subset. Furthermore, PSP secreted higher levels of the immunosuppressive cytokine IL-10 than children who progressed. The frequency of suppressive TREG, CM TREG proliferation, and IL-10 production were all lower in PSP who go on to progress at a later time-point, supporting the importance of an active TREG response in preventing disease progression. In addition, we find that IL-7 homeostatic signaling is enhanced in PSP, both through preserved surface IL-7receptor (CD127) expression on central memory T-cells and increased plasma levels of soluble IL-7receptor, which enhances the bioactivity of IL-7. Combined analysis, using a LASSO modeling approach, indicates that both TREG activity and homeostatic T-cell signaling make independent contributions to the preservation of CD4 T-cells in HIV-infected children. Together, these data demonstrate that maintenance of normal-for-age CD4 counts in PSP is an active process, which requires both suppression of immune activation through functional TREG, and enhanced T-cell homeostatic signaling.
Keywords: homeostatic signaling; IL-10; IL-7; immune activation (IA); immune regulation; pediatric HIV-infection; pediatric slow progression; regulatory T cells (Treg).
Figures
References
-
- Blanche S, Newell ML, Mayaux MJ, Dunn DT, Teglas JP, Rouzioux C, et al. Morbidity and mortality in European children vertically infected by HIV-1. The french pediatric HIV infection study group and european collaborative study. J Acquir Immune Defic Syndr Hum Retrovirol. (1997) 14:442–50 - PubMed
-
- Ananworanich J, Apornpong T, Kosalaraksa P, Jaimulwong T, Hansudewechakul R, Pancharoen C, et al. Characteristics of lymphocyte subsets in HIV-infected, long-term nonprogressor, and healthy Asian children through 12 years of age. J Allergy Clin Immunol. (2010) 126:1294–1301 e1210. 10.1016/j.jaci.2010.09.038 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous