

Transient Elastography and Ultrasonography: Optimal Evaluation of Liver Fibrosis and Cirrhosis in Patients with Chronic Hepatitis B Concurrent with Nonalcoholic Fatty Liver Disease
- PMID: 30809540
- PMCID: PMC6364122
- DOI: 10.1155/2019/3951574
Transient Elastography and Ultrasonography: Optimal Evaluation of Liver Fibrosis and Cirrhosis in Patients with Chronic Hepatitis B Concurrent with Nonalcoholic Fatty Liver Disease
Abstract
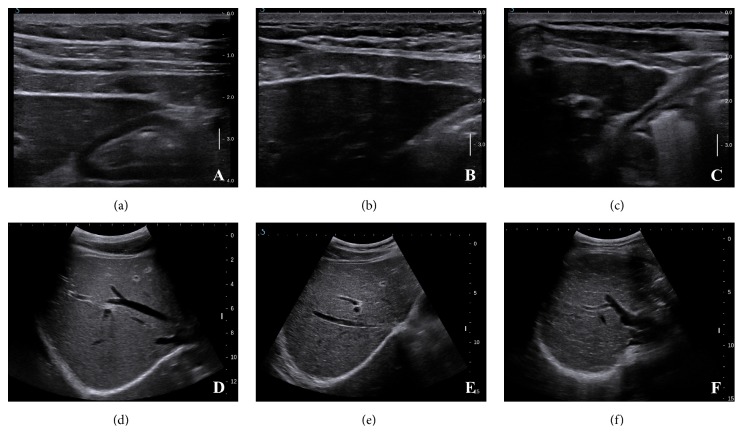
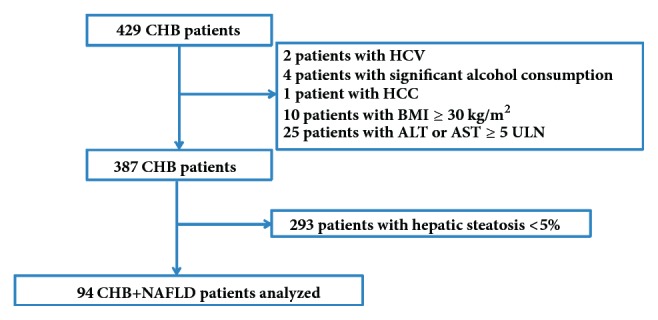
Background and aims: Concordance between transient elastography (TE) and ultrasonography (US) in assessing liver fibrosis in patients with chronic hepatitis B (CHB) and concurrent nonalcoholic fatty liver disease (NAFLD) has been rarely studied. This study aimed to evaluate the individual and combined performances of TE and US in assessing liver fibrosis and cirrhosis.
Patients and methods: Consecutive CHB patients with NAFLD were prospectively enrolled. TE and US examinations were performed, with liver biopsy as a reference standard. Receiver operating characteristic (ROC) curves were obtained to evaluate the diagnostic performance. Differences between the areas under the ROC curves (AUCs) were compared using DeLong's test.
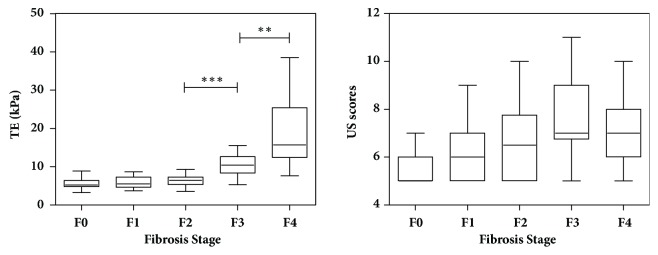
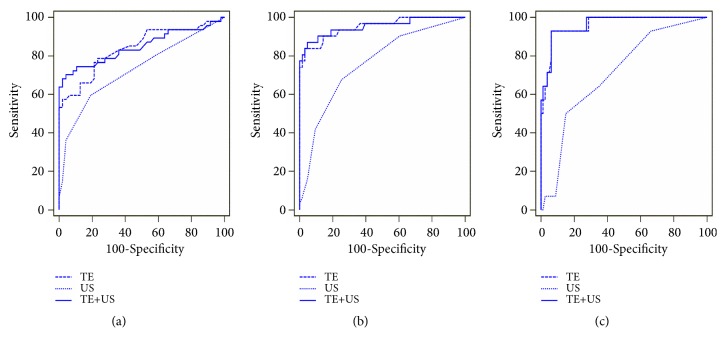
Results: TE and US scores correlated significantly with the histological fibrosis staging scores. TE was significantly superior to US in the diagnosis of significant fibrosis (AUC, 0.84 vs 0.73; P=0.02), advanced fibrosis (AUC, 0.95 vs 0.76; P<0.001), and cirrhosis (AUC, 0.96 vs 0.71; P<0.001). Combining TE with US did not increase the accuracy of detecting significant fibrosis, advanced cirrhosis, or cirrhosis (P=0.62, P=0.69, and P=0.38, respectively) compared to TE alone. However, TE combined with US significantly increased the positive predictive value for significant fibrosis when compared to TE alone. The optimal cut-off values of TE for predicting advanced fibrosis and cirrhosis were 8.7 kPa and 10.9 kPa, with negative predictive values of 92.4% and 98.7%, respectively.
Conclusions: TE is useful for predicting hepatic fibrosis and excluding cirrhosis in CHB patients with NAFLD. A combination of TE and US does not improve the accuracy in assessing liver fibrosis or cirrhosis.
Figures
References
-
- Singh S., Allen A. M., Wang Z., Prokop L. J., Murad M. H., Loomba R. Fibrosis progression in nonalcoholic fatty liver vs Nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clinical Gastroenterology and Hepatology. 2015;13(4):643–654. doi: 10.1016/j.cgh.2014.04.014. - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
