

An approach to structural facial rejuvenation with fillers in women
- PMID: 30809580
- PMCID: PMC6374711
- DOI: 10.1016/j.ijwd.2018.08.011
An approach to structural facial rejuvenation with fillers in women
Abstract
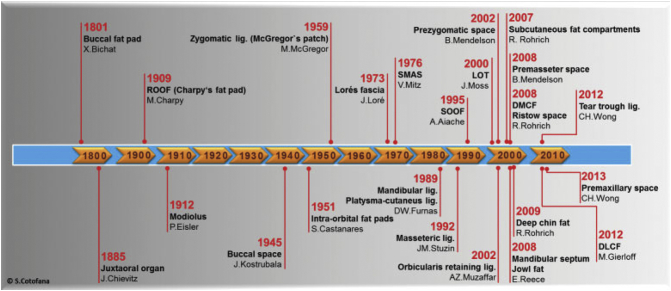
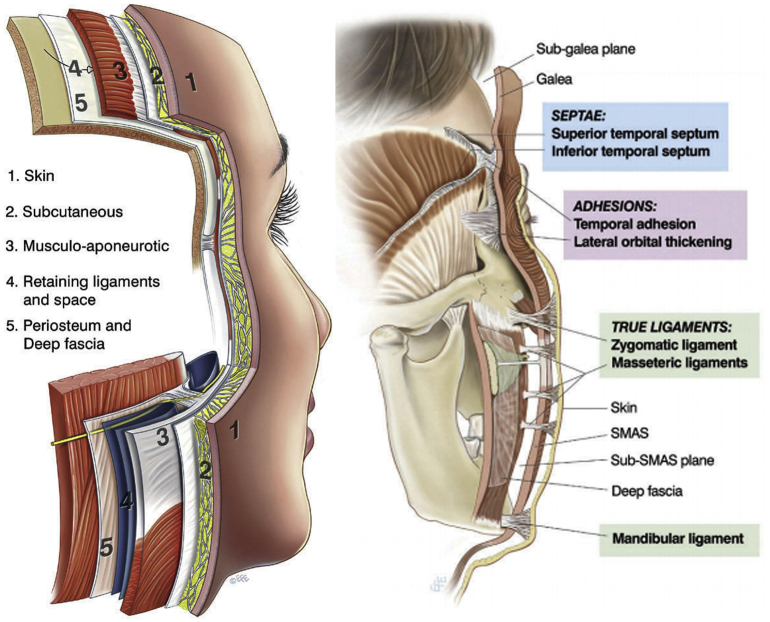
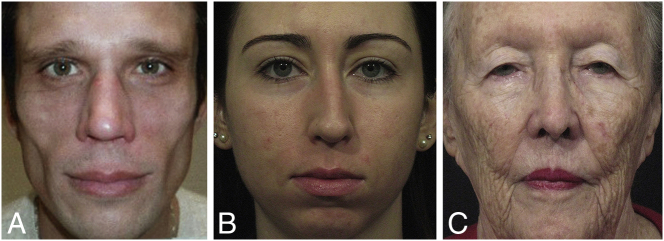
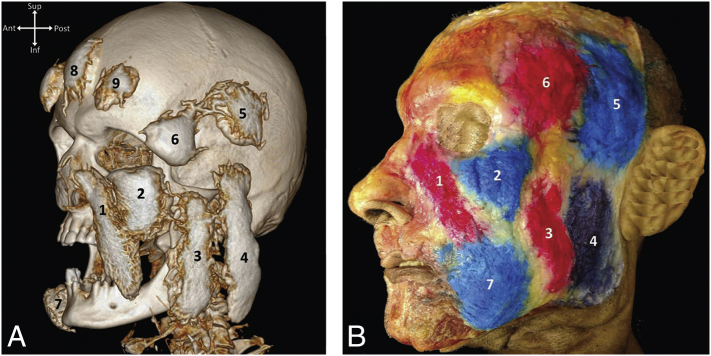
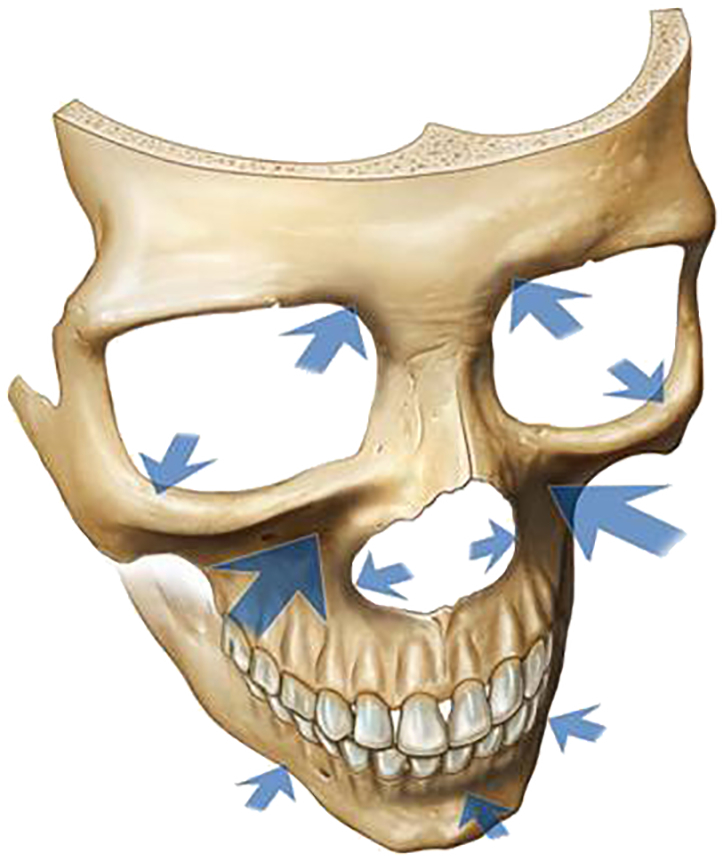
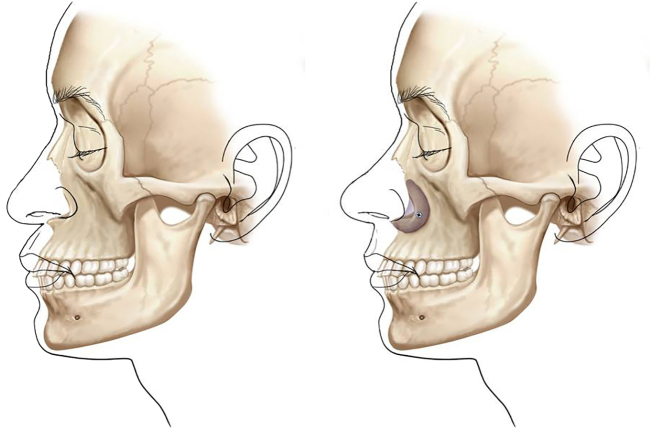
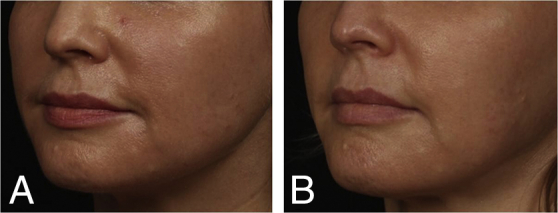
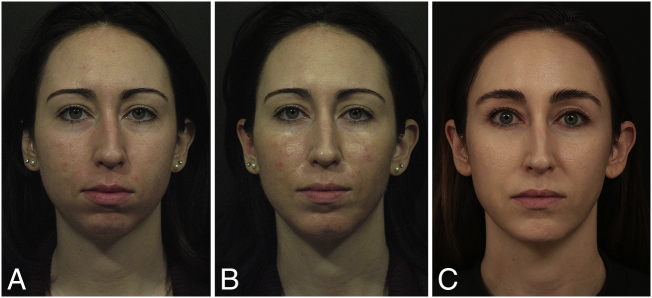
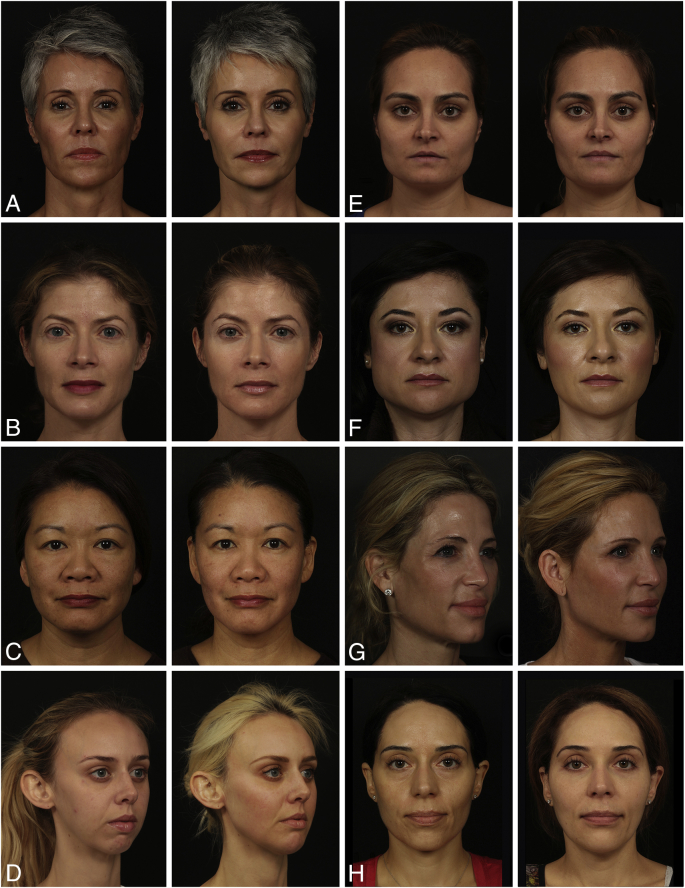
Newer understanding of volume loss as a critical component of facial aging and the integration of volume replacement into the surgical and nonsurgical therapeutic algorithm is arguably the most significant recent development in the field of facial rejuvenation. As all structural tissues play a role in the aging face, restoring youthful characteristics (or establishing them where they are congenitally absent) starts from the skeletal framework and builds progressively to the canvas of the face. The purpose of this article is to provide an introduction and brief summary of some of the current concepts concerning facial anatomy and the anatomy of facial aging, which serve as the basis for predictable and reproducible results with the use of injectable fillers. This article does not include the various types of fillers or techniques of filler injection, but covers how to decide where to use the filler and why, in different faces, as a result of the recognition and targeted correction of currently recognized specific anatomic deficiencies.
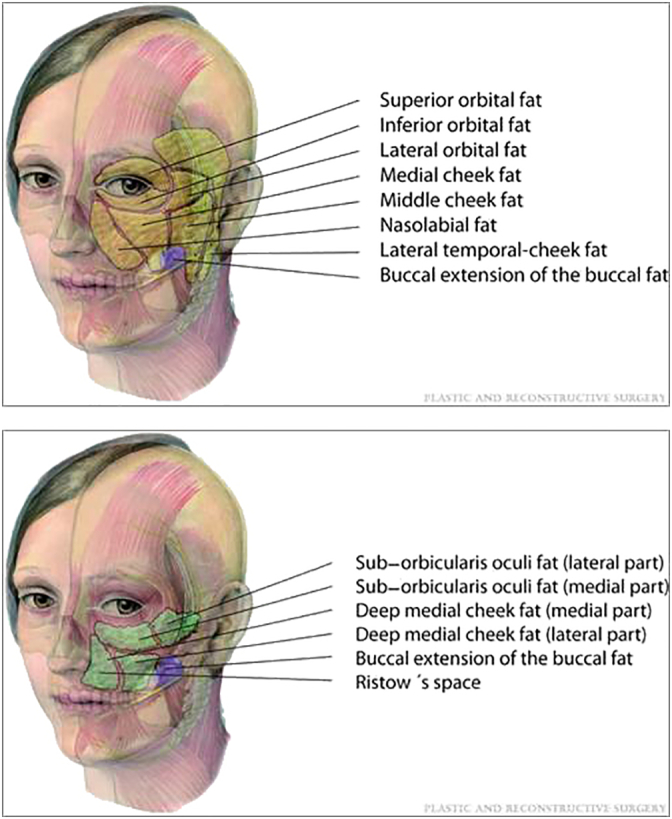
Keywords: Filler placement; anatomy of aging; facial analysis; facial fat compartments; facial volumization.
Figures




References
-
- Avelar L.E., Cazerta C.E., Ave M.N., Shitara D.I. Dynamic changes of facial supporting cornerstones (pillars): Considerations in aesthetic approach. J Drugs Dermatol. 2018;17(4):466–470. - PubMed
-
- Azizzadeh B., Murphy M., Johnson C. Elsevier; 2007. Master techniques in facial rejuvenation.
-
- Azizzadeh B., Murphy M., Johnson C., Massry G., Fitzgerald R. Elsevier; London: 2018. Master techniques in facial rejuvenation.
-
- Bashour M. History and current concepts in the analysis of facial attractiveness. Plast Reconstr Surg. 2006;118:741–756. - PubMed
-
- Cotofana S., Schenck T.L., Trevidic P. Midface: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136.5S:219S–234S. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
