

The rise and fall of long-latency Plasmodium vivax
- PMID: 30809676
- PMCID: PMC6432802
- DOI: 10.1093/trstmh/trz002
The rise and fall of long-latency Plasmodium vivax
Abstract
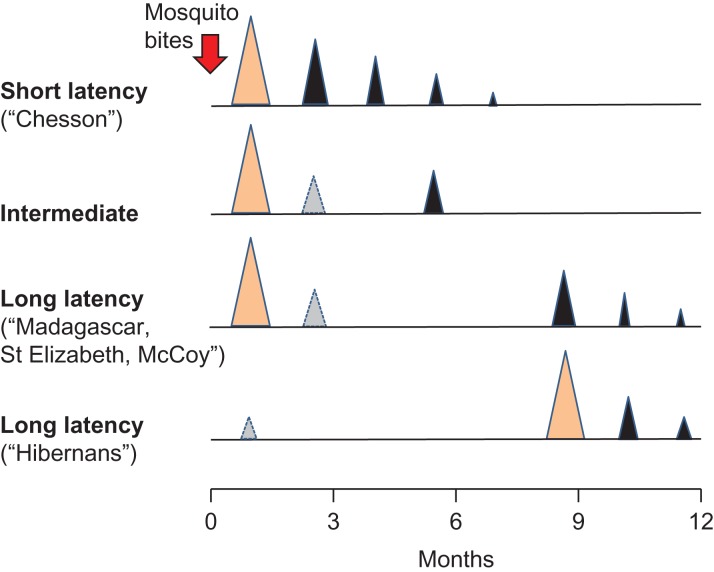
Until World War II the only clinical phenotype of Plasmodium vivax generally recognised in medicine was one associated with either a long (8-9 months) incubation period or a similarly long interval between initial illness and the first relapse. Long-latency P. vivax 'strains' were the first in which relapse, drug resistance and pre-erythrocytic development were described. They were the infections in which primaquine radical cure dosing was developed. A long-latency 'strain' was the first to be fully sequenced. Although long-latency P. vivax is still present in some parts of Asia, North Africa and the Americas, in recent years it has been largely forgotten.
Keywords: Plasmodium vivax; long latency; malaria; relapse.
© The Author(s) 2019. Published by Oxford University Press on behalf of Royal Society of Tropical Medicine and Hygiene.
Figures
References
-
- Yorke W, MacFie JWS. Observations on malaria made during the treatment of general paralysis. Trans R Soc Trop Med Hyg 1924;18(1–2):13–37.
-
- Wagner-Jauregg J. Die Behandlung der progressiven Paralyse und Tabes. Wien Med Wochenschr 1921;71:1105–9, 1209–15. - PubMed
-
- Snounou G, Pérignon JL. Malariotherapy—insanity at the service of malariology. Adv Parasitol 2013;81:223–55. - PubMed
-
- Yorke W. Further observations on malaria made during the treatment of general paralysis. Trans R Soc Trop Med Hyg 1926;19(3):108–22.
