

Survival Differences in Women and Men After Septal Myectomy for Obstructive Hypertrophic Cardiomyopathy
- PMID: 30810698
- PMCID: PMC6439557
- DOI: 10.1001/jamacardio.2019.0084
Survival Differences in Women and Men After Septal Myectomy for Obstructive Hypertrophic Cardiomyopathy
Abstract
Importance: Recent data indicate that women with hypertrophic cardiomyopathy (HCM) are older and more symptomatic at presentation and have worse clinical outcomes than men. However, to our knowledge, there are no large studies of the association of patient sex with outcomes after surgical myectomy.
Objective: To analyze preoperative characteristics and overall survival of women and men undergoing septal myectomy for obstructive HCM.
Design, setting, and participants: This retrospective, single-center study included the clinical data of adult patients who underwent septal myectomy from January 1961 through April 2016. Data analysis occurred from December 2017 to December 2018.
Exposures: Septal myectomy.
Main outcomes and measures: Survival.
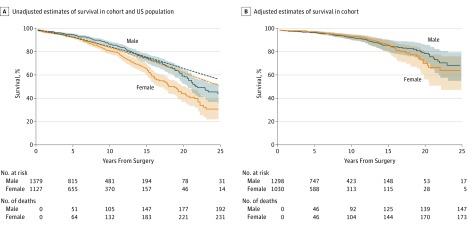
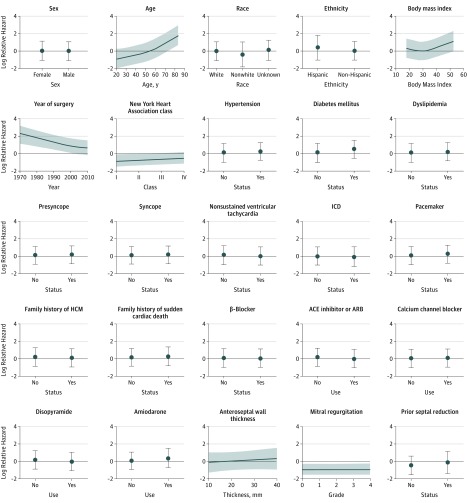
Results: A total of 2506 adults were included; 1379 patients (55.0%) were men. At the time of surgery, women were older, with median (IQR) age of 59.5 (46.6-68.2) years vs 52.9 (42.9-62.7) years in men (P < .001). Women were more likely to have New York Heart Association class III or IV status at presentation (women, 1023 [90.8%]; men, 1169 [84.8%]; P < .001) and more severe obstructive physiology, as reflected in higher resting left ventricular outflow tract gradients (women, 67.0 [36.0-97.0] mm Hg; men, 50.0 [23.0-81.0] mm Hg; P < .001). Women also had a greater likelihood of having moderate or severe mitral regurgitation (606 [55.2%]) than men (581 [43.1%]; P < .001) and higher right ventricular systolic pressure (women, 36.0 [30.0-46.0] mm Hg; men, 33.0 [28.0-39.0] mm Hg; P < .001). The unadjusted overall survival was lower in women, corresponding to a median 3.9-year shorter survival than men (median [IQR] survival time: women, 18.2 [12.1-27.2] years; men, 22.1 [15.1-32.5] years; P < .001). In a multivariable Cox regression analysis, however, the association between sex and mortality was attenuated and not significant after controlling for other baseline variables (hazard ratio, 0.98 [95% CI, 0.76-1.26]; P = .86). Among the covariates in the model, older age at surgery (adjusted hazard ratio [aHR], 3.09 [95% CI, 2.12-4.52]; P < .001), higher body mass index (aHR, 1.22 [95% CI, 0.90-1.66]; P < .001), greater NYHA class (aHR, 2.31 [95% CI, 1.03-5.15]; P = .04), and presence of diabetes prior to surgery (aHR, 1.57 [95% CI, 1.10-2.24]; P = .01) were each independently associated with increased mortality. Operations performed later in the study period (2013 vs 2004) were associated with decreased mortality (aHR, 0.82 [95% CI, 0.55-1.22]; P = .001).
Conclusions and relevance: In this large cohort of surgical patients with obstructive HCM, we observed significant differences at clinical presentation between women and men, in that women were older and more symptomatic. However, after adjustment for important baseline prognostic factors, there was no survival difference after septal myectomy by sex. Improved care of women with obstructive HCM should focus on early identification of disease and prompt surgical referral of appropriate patients who do not respond to medical treatment.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
