

Baseline Characteristics and Risk Profiles of Participants in the ISCHEMIA Randomized Clinical Trial
- PMID: 30810700
- PMCID: PMC6439551
- DOI: 10.1001/jamacardio.2019.0014
Baseline Characteristics and Risk Profiles of Participants in the ISCHEMIA Randomized Clinical Trial
Erratum in
-
Errors in Group Information and Additional Contributions.JAMA Cardiol. 2019 May 1;4(5):497. doi: 10.1001/jamacardio.2019.0866. JAMA Cardiol. 2019. PMID: 30969313 Free PMC article. No abstract available.
Abstract
Importance: It is unknown whether coronary revascularization, when added to optimal medical therapy, improves prognosis in patients with stable ischemic heart disease (SIHD) at increased risk of cardiovascular events owing to moderate or severe ischemia.
Objective: To describe baseline characteristics of participants enrolled and randomized in the International Study of Comparative Health Effectiveness With Medical and Invasive Approaches (ISCHEMIA) trial and to evaluate whether qualification by stress imaging or nonimaging exercise tolerance test (ETT) influenced risk profiles.
Design, setting, and participants: The ISCHEMIA trial recruited patients with SIHD with moderate or severe ischemia on stress testing. Blinded coronary computed tomography angiography was performed in most participants and reviewed by a core laboratory to exclude left main stenosis of at least 50% or no obstructive coronary artery disease (CAD) (<50% for imaging stress test and <70% for ETT). The study included 341 enrolling sites (320 randomizing) in 38 countries and patients with SIHD and moderate or severe ischemia on stress testing. Data presented were extracted on December 17, 2018.
Main outcomes and measures: Enrolled, excluded, and randomized participants' baseline characteristics. No clinical outcomes are reported.
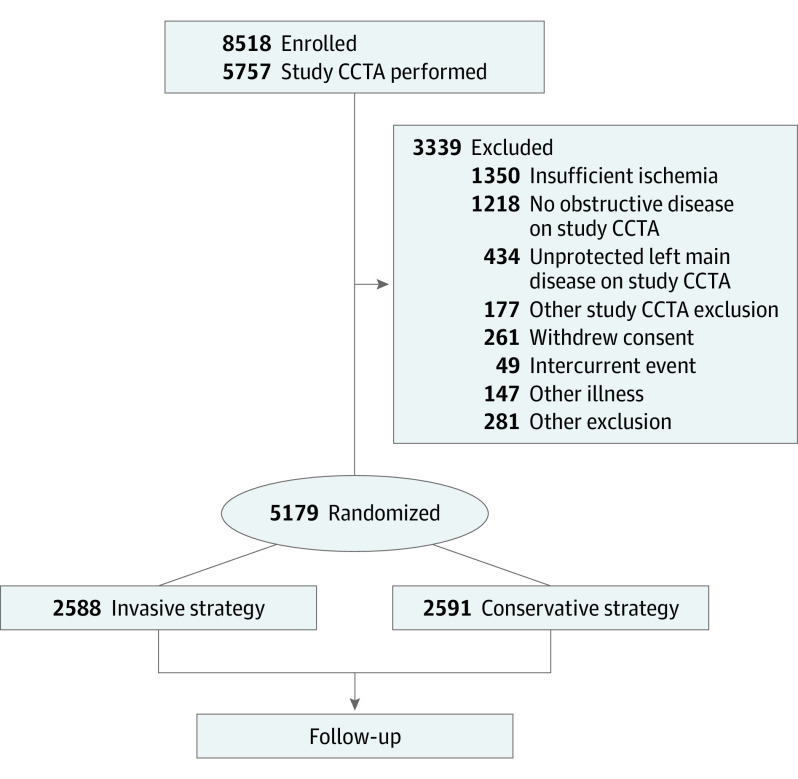
Results: A total of 8518 patients were enrolled, and 5179 were randomized. Common reasons for exclusion were core laboratory determination of insufficient ischemia, unprotected left main stenosis of at least 50%, or no stenosis that met study obstructive CAD criteria on study coronary computed tomography angiography. Randomized participants had a median age of 64 years, with 1168 women (22.6%), 1726 nonwhite participants (33.7%), 748 Hispanic participants (15.5%), 2122 with diabetes (41.0%), and 4643 with a history of angina (89.7%). Among the 3909 participants randomized after stress imaging, core laboratory assessment of ischemia severity (in 3901 participants) was severe in 1748 (44.8%), moderate in 1600 (41.0%), mild in 317 (8.1%) and none or uninterpretable in 236 (6.0%), Among the 1270 participants who were randomized after nonimaging ETT, core laboratory determination of ischemia severity (in 1266 participants) was severe (an eligibility criterion) in 1051 (83.0%), moderate in 101 (8.0%), mild in 34 (2.7%) and none or uninterpretable in 80 (6.3%). Among the 3912 of 5179 randomized participants who underwent coronary computed tomography angiography, 79.0% had multivessel CAD (n = 2679 of 3390) and 86.8% had left anterior descending (LAD) stenosis (n = 3190 of 3677) (proximal in 46.8% [n = 1749 of 3739]). Participants undergoing ETT had greater frequency of 3-vessel CAD, LAD, and proximal LAD stenosis than participants undergoing stress imaging.
Conclusions and relevance: The ISCHEMIA trial randomized an SIHD population with moderate or severe ischemia on stress testing, of whom most had multivessel CAD.
Trial registration: ClinicalTrials.gov Identifier: NCT01471522.
Conflict of interest statement
Figures
Comment in
-
Is the Search for Enough Moderate-Severe Ischemia Nearly Over?JAMA Cardiol. 2019 Mar 1;4(3):203-205. doi: 10.1001/jamacardio.2019.0024. JAMA Cardiol. 2019. PMID: 30810699 No abstract available.
References
-
- Shaw LJ, Berman DS, Picard MH, et al. ; National Institutes of Health/National Heart, Lung, and Blood Institute-Sponsored ISCHEMIA Trial Investigators . Comparative definitions for moderate-severe ischemia in stress nuclear, echocardiography, and magnetic resonance imaging. JACC Cardiovasc Imaging. 2014;7(6):593-604. doi: 10.1016/j.jcmg.2013.10.021 - DOI - PMC - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
