

Treatment of a calcific bursitis of the medial collateral ligament: a rare cause of painful knee
- PMID: 30811015
- PMCID: PMC6838279
- DOI: 10.1007/s40477-018-0353-y
Treatment of a calcific bursitis of the medial collateral ligament: a rare cause of painful knee
Abstract
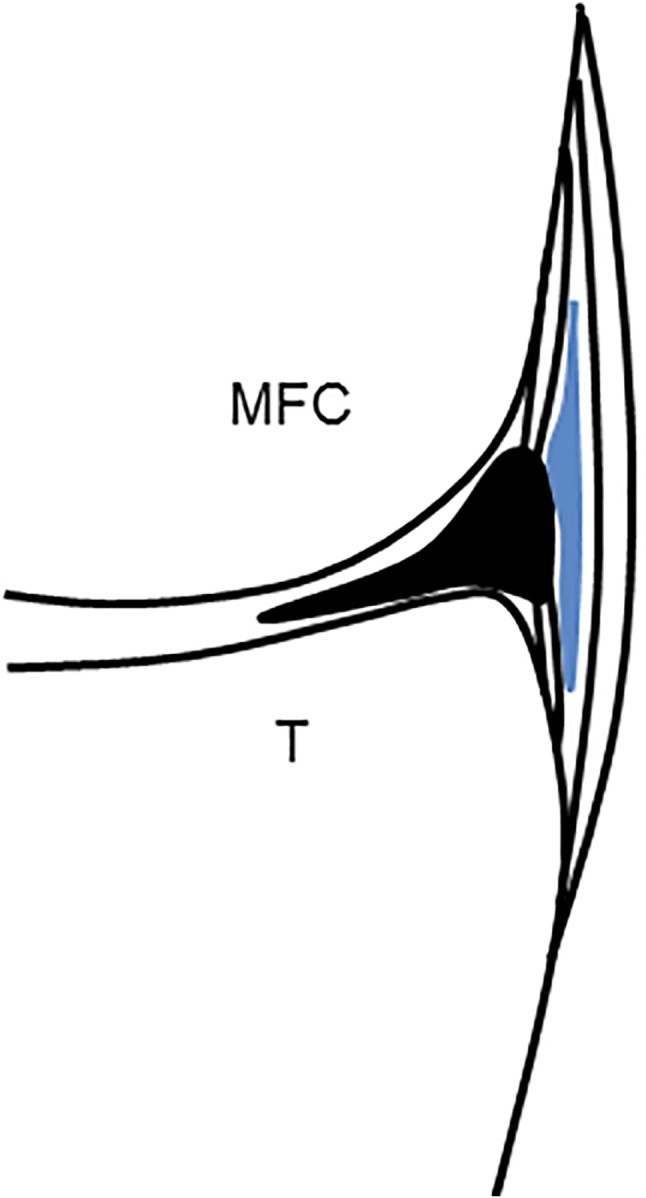
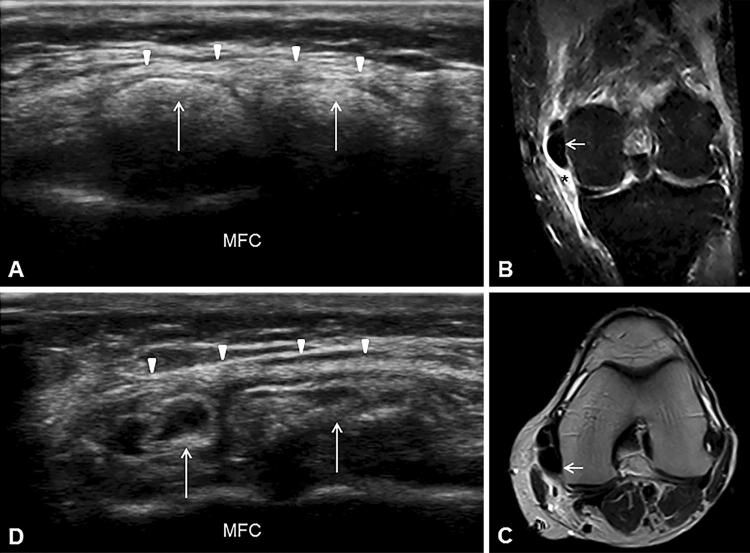
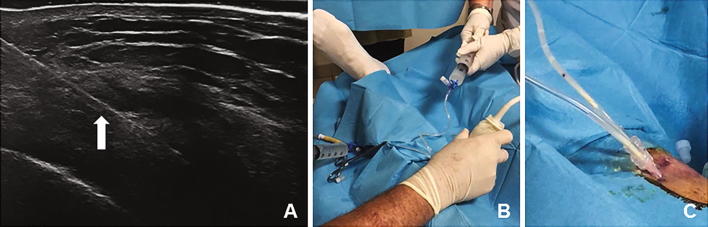
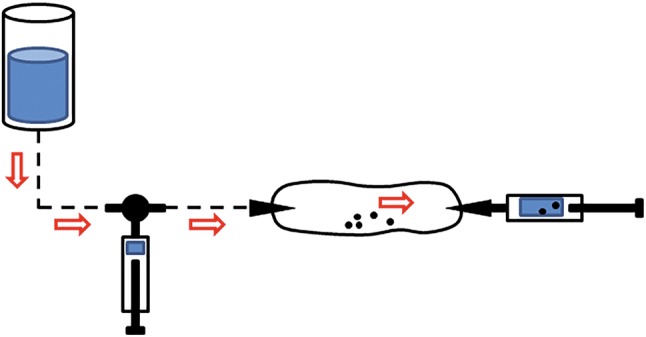
Medial knee pain is common in clinical practice and can be caused by various conditions. In rare cases, it can even be by calcific bursitis of the medial collateral ligament (MCL). Treatment of calcific bursitis and/or calcification of the MCL classically includes observation, local injections, shockwave therapy and surgical resection. We report a case of nontraumatic medial knee pain poorly responsive to conservative treatments. Ultrasound (US) imaging revealed a massive lobed hyperechoic formation with partial acoustic shadow in the MCL context compatible with calcific bursitis, and magnetic resonance imaging (MRI) confirmed the presence of the bursa's calcific deposit surrounded by hyperintense signal compatible with pericalcific edema. We performed a double-needle ultrasound-guided percutaneous lavage (UGPL), which is today a fairly common treatment for many musculoskeletal disorders, such as rotator cuff calcific tendinopathy and elbow extensor tendons pathology, but regarding the knee, it is not part of ordinary care. This report shows the clinical and imaging presentation of calcific bursitis of the MCL and describes in detail the technique to perform the UGPL with a system of two needles, two syringes and a double connection to ensure a correct lavage of the calcium deposit without significant intrabursal pressure increase and consequently without pain during the procedure.
Il dolore localizzato alla regione mediale del ginocchio è di frequente riscontro nella pratica clinica e può essere causato da diverse condizioni patologiche, in rari casi anche da una borsite calcifica del legamento collaterale mediale (LCM). Il trattamento di una borsite calcifica e/o di una calcificazione del LCM prevede classicamente il monitoraggio clinico, le infiltrazioni locali, la terapia con onde d’urto ed infine la rimozione chirurgica. Riportiamo un caso di dolore localizzato alla regione mediale del ginocchio, non traumatico, scarsamente responsivo ai trattamenti conservativi. La valutazione ecografica ha rivelato la presenza di una voluminosa formazione iperecogena polilobata con parziale cono d’ombra posteriore nel contesto del LCM, compatibile con una borsite calcifica intra-ligamentosa; le scansioni di risonanza magnetica nucleare (RMN) hanno confermato la presenza del deposito endo-bursale circondato da segnale iperintenso compatibile con edema peri-calcifico. Abbiamo quindi eseguito una procedura di lavaggio percutaneo eco-guidato con due aghi, che ad oggi rappresenta un trattamento ampiamente utilizzato per diverse patologie del sistema muscolo scheletrico come la tendinopatia calcifica della cuffia dei rotatori della spalla e la patologia calcifica degli estensori di gomito, mentre per il ginocchio non rientra nei trattamenti eseguiti di routine. Questo articolo illustra le caratteristiche cliniche ed ecografiche della borsite calcifica del LCM ed ha l’obiettivo di descrivere in dettaglio la tecnica per eseguire un lavaggio percutaneo eco-guidato con un sistema di due aghi, due siringhe e un duplice tubo di raccordo per assicurare un completo lavaggio del deposito calcifico senza significativo aumento della pressione intra-bursale con l’obiettivo di minimizzare il dolore in corso di procedura.
Keywords: Calcific bursitis; Medial collateral ligament; Pain; Treatment; Ultrasound; Voshell’s bursa.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
