

Improving preterm newborn identification in low-resource settings with machine learning
- PMID: 30811399
- PMCID: PMC6392324
- DOI: 10.1371/journal.pone.0198919
Improving preterm newborn identification in low-resource settings with machine learning
Abstract
Background: Globally, preterm birth is the leading cause of neonatal death with estimated prevalence and associated mortality highest in low- and middle-income countries (LMICs). Accurate identification of preterm infants is important at the individual level for appropriate clinical intervention as well as at the population level for informed policy decisions and resource allocation. As early prenatal ultrasound is commonly not available in these settings, gestational age (GA) is often estimated using newborn assessment at birth. This approach assumes last menstrual period to be unreliable and birthweight to be unable to distinguish preterm infants from those that are small for gestational age (SGA). We sought to leverage machine learning algorithms incorporating maternal factors associated with SGA to improve accuracy of preterm newborn identification in LMIC settings.
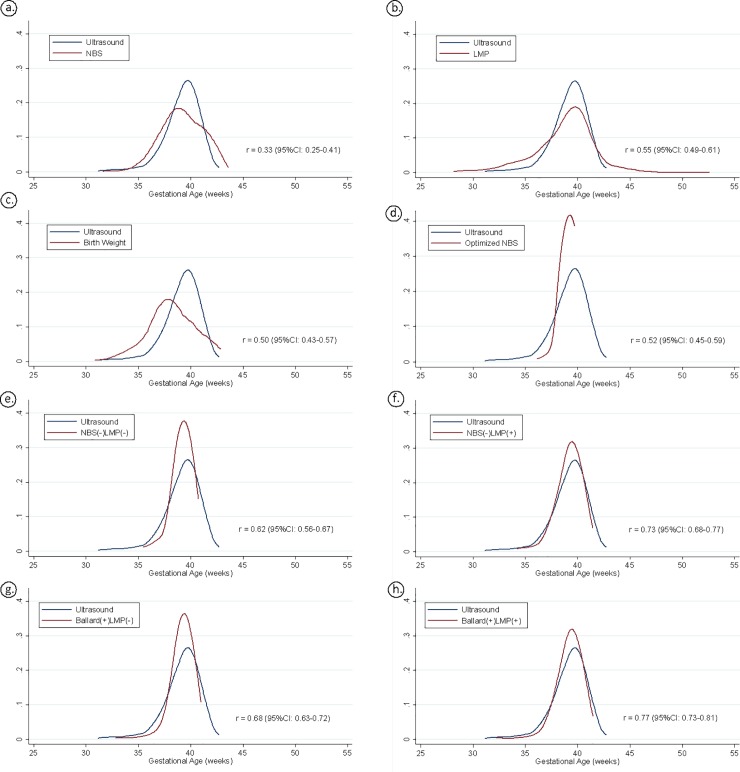
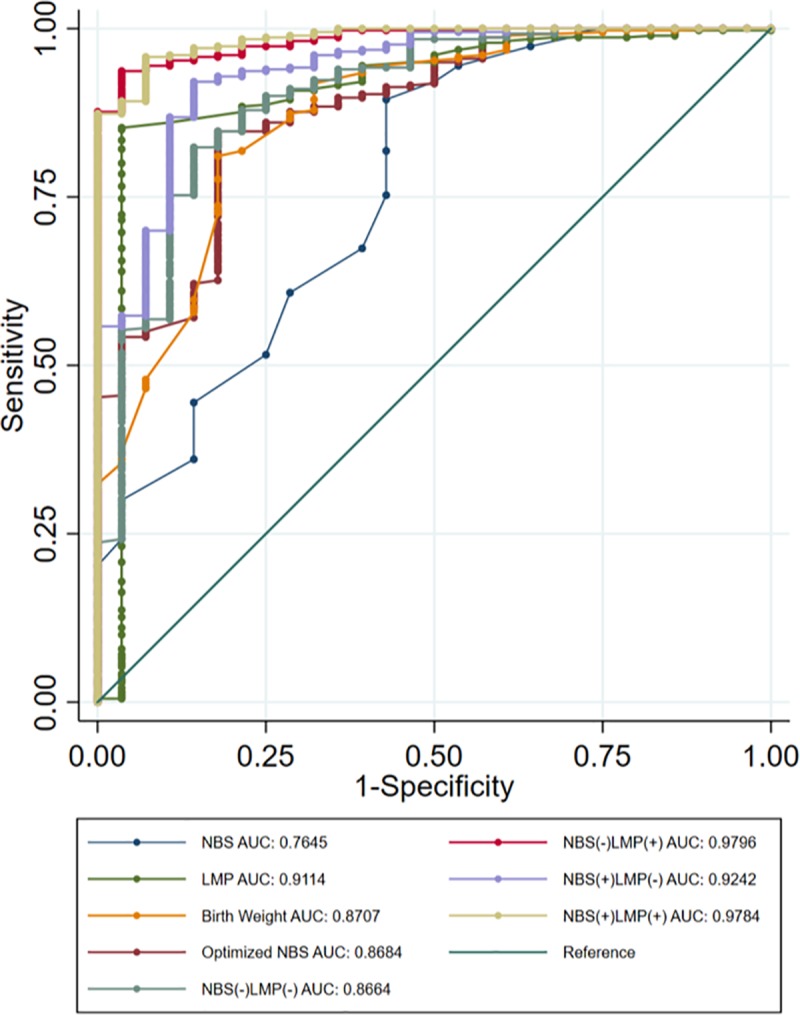
Methods and findings: This study uses data from an ongoing obstetrical cohort in Lusaka, Zambia that uses early pregnancy ultrasound to estimate GA. Our intent was to identify the best set of parameters commonly available at delivery to correctly categorize births as either preterm (<37 weeks) or term, compared to GA assigned by early ultrasound as the gold standard. Trained midwives conducted a newborn assessment (<72 hours) and collected maternal and neonatal data at the time of delivery or shortly thereafter. New Ballard Score (NBS), last menstrual period (LMP), and birth weight were used individually to assign GA at delivery and categorize each birth as either preterm or term. Additionally, machine learning techniques incorporated combinations of these measures with several maternal and newborn characteristics associated with prematurity and SGA to develop GA at delivery and preterm birth prediction models. The distribution and accuracy of all models were compared to early ultrasound dating. Within our live-born cohort to date (n = 862), the median GA at delivery by early ultrasound was 39.4 weeks (IQR: 38.3-40.3). Among assessed newborns with complete data included in this analysis (n = 468), the median GA by ultrasound was 39.6 weeks (IQR: 38.4-40.3). Using machine learning, we identified a combination of six accessible parameters (LMP, birth weight, twin delivery, maternal height, hypertension in labor, and HIV serostatus) that can be used by machine learning to outperform current GA prediction methods. For preterm birth prediction, this combination of covariates correctly classified >94% of newborns and achieved an area under the curve (AUC) of 0.9796.
Conclusions: We identified a parsimonious list of variables that can be used by machine learning approaches to improve accuracy of preterm newborn identification. Our best-performing model included LMP, birth weight, twin delivery, HIV serostatus, and maternal factors associated with SGA. These variables are all easily collected at delivery, reducing the skill and time required by the frontline health worker to assess GA.
Trial registration: ClinicalTrials.gov Identifier: NCT02738892.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Machine learning guided postnatal gestational age assessment using new-born screening metabolomic data in South Asia and sub-Saharan Africa.BMC Pregnancy Childbirth. 2021 Sep 7;21(1):609. doi: 10.1186/s12884-021-04067-y. BMC Pregnancy Childbirth. 2021. PMID: 34493237 Free PMC article.
-
Newborn Skin Maturity Medical Device Validation for Gestational Age Prediction: Clinical Trial.J Med Internet Res. 2022 Sep 7;24(9):e38727. doi: 10.2196/38727. J Med Internet Res. 2022. PMID: 36069805 Free PMC article.
-
Simplified models to assess newborn gestational age in low-middle income countries: findings from a multicountry, prospective cohort study.BMJ Glob Health. 2021 Sep;6(9):e005688. doi: 10.1136/bmjgh-2021-005688. BMJ Glob Health. 2021. PMID: 34518201 Free PMC article.
-
Influence of different methods for calculating gestational age at birth on prematurity and small for gestational age proportions: a systematic review with meta-analysis.BMC Pregnancy Childbirth. 2023 Feb 11;23(1):106. doi: 10.1186/s12884-023-05411-0. BMC Pregnancy Childbirth. 2023. PMID: 36774458 Free PMC article.
-
New Option in the Lives Saved Tool (LiST) Allows for the Conversion of Prevalence of Small-for-Gestational-Age and Preterm Births to Prevalence of Low Birth Weight.J Nutr. 2017 Nov;147(11):2141S-2146S. doi: 10.3945/jn.117.247767. Epub 2017 Sep 13. J Nutr. 2017. PMID: 28904115 Review.
Cited by
-
Development and external validation of machine learning algorithms for postnatal gestational age estimation using clinical data and metabolomic markers.PLoS One. 2023 Mar 6;18(3):e0281074. doi: 10.1371/journal.pone.0281074. eCollection 2023. PLoS One. 2023. PMID: 36877673 Free PMC article.
-
Applications of artificial intelligence in obstetrics.Ultrasonography. 2023 Jan;42(1):2-9. doi: 10.14366/usg.22063. Epub 2022 Jul 20. Ultrasonography. 2023. PMID: 36588179 Free PMC article.
-
Artificial intelligence and the future of global health.Lancet. 2020 May 16;395(10236):1579-1586. doi: 10.1016/S0140-6736(20)30226-9. Lancet. 2020. PMID: 32416782 Free PMC article. Review.
-
Gestational age assessed by optical skin reflection in low-birth-weight newborns: Applications in classification at birth.Front Pediatr. 2023 Mar 28;11:1141894. doi: 10.3389/fped.2023.1141894. eCollection 2023. Front Pediatr. 2023. PMID: 37056944 Free PMC article.
-
Predicting preterm birth using explainable machine learning in a prospective cohort of nulliparous and multiparous pregnant women.PLoS One. 2023 Dec 27;18(12):e0293925. doi: 10.1371/journal.pone.0293925. eCollection 2023. PLoS One. 2023. PMID: 38150456 Free PMC article.
References
-
- Blencowe H, Cousens S, Oestergaard MZ, Chou D, Moller AB, Narwal R, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. Lancet. 2012;379(9832):2162–72. 10.1016/S0140-6736(12)60820-4 - DOI - PubMed
-
- Wang ML, Dorer DJ, Fleming MP, Catlin EA. Clinical outcomes of near-term infants. Pediatrics. 2004;114(2):372–6. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
