

Factors Influencing Optical Coherence Tomography Peripapillary Choroidal Thickness: A Multicenter Study
- PMID: 30811523
- PMCID: PMC6392476
- DOI: 10.1167/iovs.18-25407
Factors Influencing Optical Coherence Tomography Peripapillary Choroidal Thickness: A Multicenter Study
Abstract
Purpose: To quantify peripapillary choroidal thickness (PCT) and the factors that influence it in healthy participants who represent the racial and ethnic composition of the U.S. population.
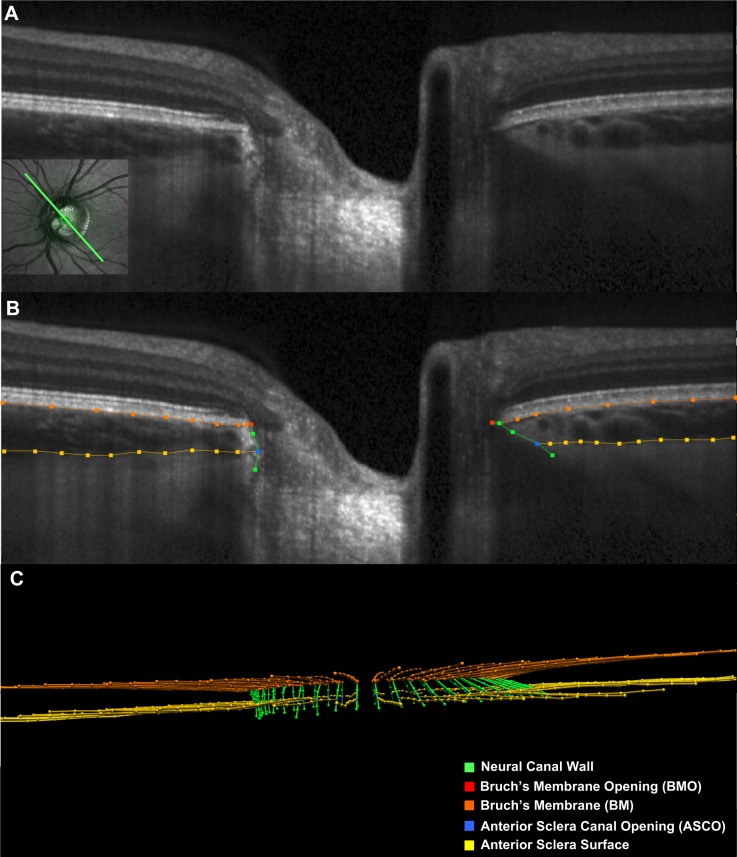
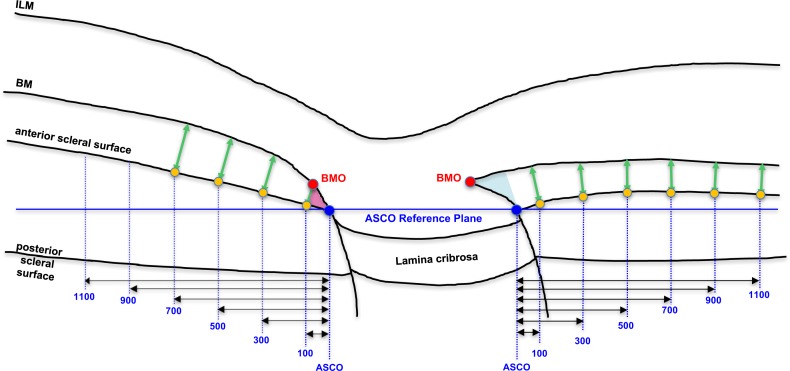
Methods: A total of 362 healthy participants underwent optical coherence tomography (OCT) enhanced depth imaging of the optic nerve head with a 24 radial B-scan pattern aligned to the fovea to Bruch's membrane opening axis. Bruch's membrane, anterior scleral canal opening (ASCO), and the anterior scleral surface were manually segmented. PCT was measured at 100, 300, 500, 700, 900, and 1100 μm from the ASCO globally and within 12 clock-hour sectors. The effects of age, axial length, intraocular pressure, ethnicity, sex, sector, and ASCO area on PCT were assessed by ANOVA and univariable and multivariable regressions.
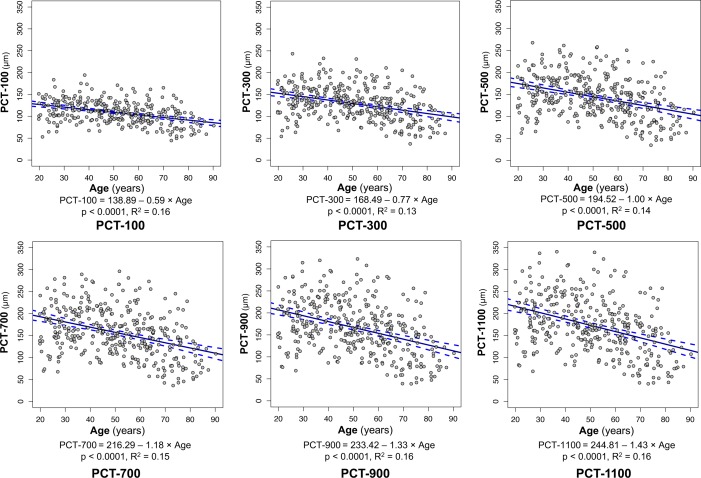
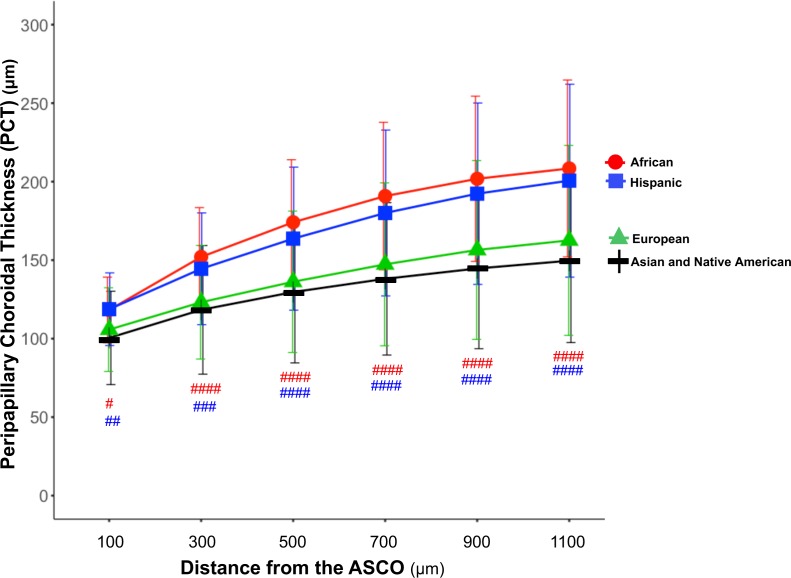
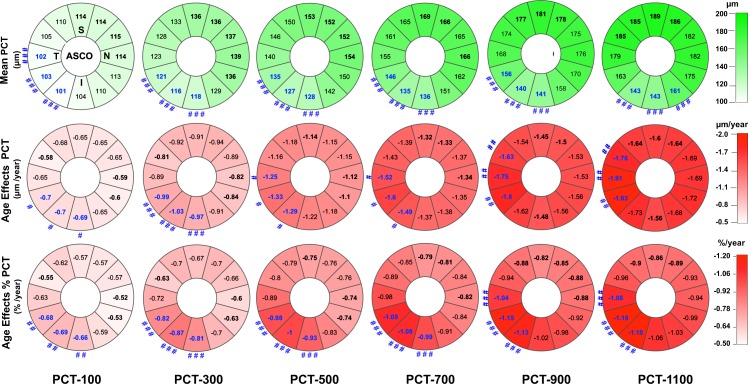
Results: Globally, PCT was thicker further from the ASCO border and thinner with older age, longer axial length, larger ASCO area, European descent, and female sex. Among these effectors, age and axial length explained the greatest proportion of variance. The rate of age-related decline increased further from the ASCO border. Sectorally, the inferior-temporal sectors were thinnest (10.7%-20.0% thinner than the thickest sector) and demonstrated a higher rate of age-related loss (from 15.6% to 20.7% faster) at each ASCO distance.
Conclusions: In healthy eyes, PCT was thinnest in the inferior temporal sectors and thinner PCT was associated with older age, European descent, longer axial length, larger ASCO area, and female sex. Among these associations, age had the strongest influence, and its effect was greatest within the inferior temporal sectors.
Figures
References
-
- Hayreh SS, Jonas JB, Zimmerman MB. Parapapillary chorioretinal atrophy in chronic high-pressure experimental glaucoma in rhesus monkeys. Invest Ophthalmol Vis Sci. 1998;39:2296–2303. - PubMed
-
- Hayreh SS, Pe'er J, Zimmerman MB. Morphologic changes in chronic high-pressure experimental glaucoma in rhesus monkeys. J Glaucoma. 1999;8:56–71. - PubMed
-
- Vianna JR, Malik R, Danthurebandara VM, et al. Beta and gamma peripapillary atrophy in myopic eyes with and without glaucoma. Invest Ophthalmol Vis Sci. 2016;57:3103–3111. - PubMed
-
- Hayashi K, Tomidokoro A, Lee KY, et al. Spectral-domain optical coherence tomography of beta-zone peripapillary atrophy: influence of myopia and glaucoma. Invest Ophthalmol Vis Sci. 2012;53:1499–1505. - PubMed
