

Exploring the utility of internal whistleblowing in healthcare via agent-based models
- PMID: 30813107
- PMCID: PMC6347952
- DOI: 10.1136/bmjopen-2018-021705
Exploring the utility of internal whistleblowing in healthcare via agent-based models
Abstract
Objective: The benefits of internal whistleblowing or speaking-up in the healthcare sector are significant. The a priori assumption that employee whistleblowing is always beneficial is, however, rarely examined. While recent research has begun to consider how the complex nature of healthcare institutions impact speaking-up rates, few have investigated the institutional processes and factors that facilitate or retard the benefits of speaking up. Here we consider how the efficacy of formal inquiries within organisations in response to employees' speaking up about their concerns affects the utility of internal whistleblowing.
Design: Using computational models, we consider how best to improve patient care through internal whistleblowing when resource and practical limitations constrain healthcare operation. We analyse the ramifications of varying organisational responses to employee concerns, given organisational and practical limitations.
Setting: Drawing on evidence from international research, we test the utility of whistleblowing policies in a variety of organisational settings. This includes institutions where whistleblowing inquiries are handled with varying rates of efficiency and accuracy.
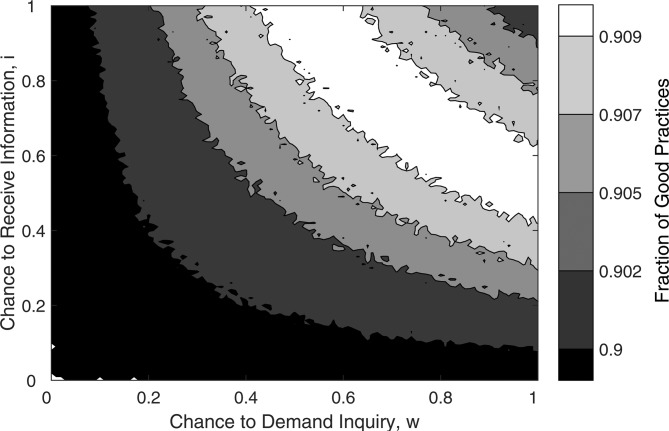
Results: We find organisational inefficiencies can negatively impact the benefits of speaking up about bad patient care. We find that, given resource limitations and review inefficiencies, it can actually improve patient care if whistleblowing rates are limited. However, we demonstrate that including softer mechanisms for internal adjustment of healthcare practice (eg, peer to peer conversation) alongside whistleblowing policy can overcome these organisational limitations.
Conclusion: Healthcare organisations internationally have a variable record of responding to employees who speak up about their workplace concerns. Where organisations get this wrong, the consequences can be serious for patient care and staff well-being. The results of this study, therefore, have implications for researchers, policy makers and healthcare organisations internationally. We conclude with a call for further research on a more holistic understanding of the interplay between organisational structure and the benefits of whistleblowing to patient care.
Keywords: health quality improvement; internal whistleblowing; raising concerns; resource limitations; simulations; speaking-up.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





References
-
- Barnett T. A preliminary investigation of the relationship between selected organizational characteristics and external whistleblowing by employees. Journal of Business Ethics 1992;11:949–59. 10.1007/BF00871961 - DOI
-
- Improvement N. Freedom to speak up: raising concerns policy for the NHS, 2016. https://improvement.nhs.uk/resources/freedom-to-speak-up-whistleblowing-....
-
- Pope-Smith A. Winterbourne View – Key Findings, Recommendations and Actions, 2011.
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous