

Emergency Medicine Palliative Care Access (EMPallA): protocol for a multicentre randomised controlled trial comparing the effectiveness of specialty outpatient versus nurse-led telephonic palliative care of older adults with advanced illness
- PMID: 30813112
- PMCID: PMC6347856
- DOI: 10.1136/bmjopen-2018-025692
Emergency Medicine Palliative Care Access (EMPallA): protocol for a multicentre randomised controlled trial comparing the effectiveness of specialty outpatient versus nurse-led telephonic palliative care of older adults with advanced illness
Abstract
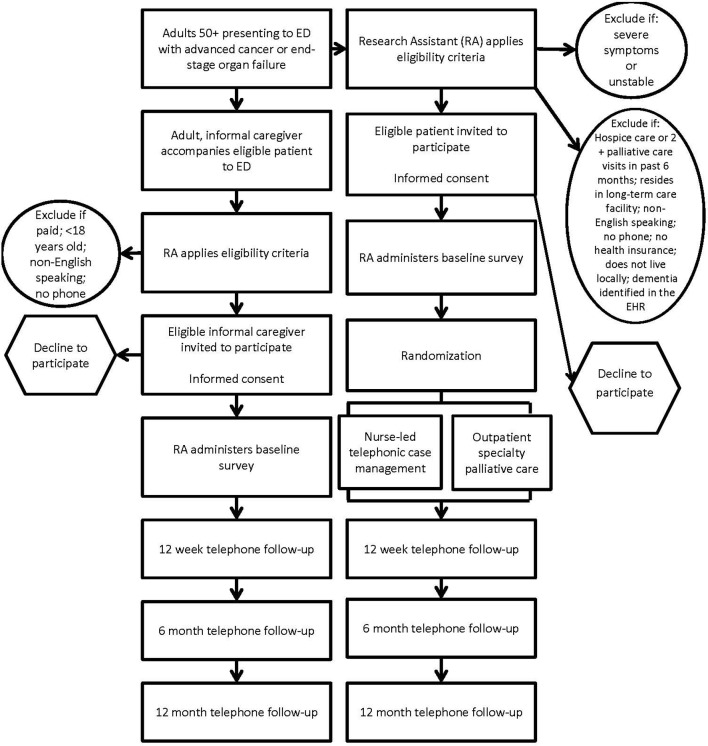
Introduction: Emergency department (ED)-initiated palliative care has been shown to improve patient-centred outcomes in older adults with serious, life-limiting illnesses. However, the optimal modality for providing such interventions is unknown. This study aims to compare nurse-led telephonic case management to specialty outpatient palliative care for older adults with serious, life-limiting illness on: (1) quality of life in patients; (2) healthcare utilisation; (3) loneliness and symptom burden and (4) caregiver strain, caregiver quality of life and bereavement.
Methods and analysis: This is a protocol for a pragmatic, multicentre, parallel, two-arm randomised controlled trial in ED patients comparing two established models of palliative care: nurse-led telephonic case management and specialty, outpatient palliative care. We will enrol 1350 patients aged 50+ years and 675 of their caregivers across nine EDs. Eligible patients: (1) have advanced cancer (metastatic solid tumour) or end-stage organ failure (New York Heart Association class III or IV heart failure, end-stage renal disease with glomerular filtration rate <15 mL/min/m2, or global initiative for chronic obstructive lung disease stage III, IV or oxygen-dependent chronic obstructive pulmonary disease); (2) speak English; (3) are scheduled for ED discharge or observation status; (4) reside locally; (5) have a working telephone and (6) are insured. Patients will be excluded if they: (1) have dementia; (2) have received hospice care or two or more palliative care visits in the last 6 months or (3) reside in a long-term care facility. We will use patient-level block randomisation, stratified by ED site and disease. Effectiveness will be compared by measuring the impact of each intervention on the specified outcomes. The primary outcome will measure change in patient quality of life.
Ethics and dissemination: Institutional Review Board approval was obtained at all study sites. Trial results will be submitted for publication in a peer-reviewed journal.
Trial registration number: NCT03325985; Pre-results.
Keywords: advanced illness; comparative effectiveness; emergency department; older adults; palliative care; randomised controlled trial.
© Author(s) (or their employer(s)) 2019. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- American Academy of Hospice and Palliative Medicine Center to Advance Palliative Care Hospice and Palliative Nurses Association Last Acts Partnership National Hospice and Palliative Care Organization. National Consensus Project for Quality Palliative Care: Clinical Practice Guidelines for quality palliative care, executive summary. J Palliat Med 2004;7:611–27. 10.1089/jpm.2004.7.611 - DOI - PubMed