

Quantitative assessment of cerebellar ataxia, through automated limb functional tests
- PMID: 30813963
- PMCID: PMC6391824
- DOI: 10.1186/s12984-019-0490-3
Quantitative assessment of cerebellar ataxia, through automated limb functional tests
Abstract
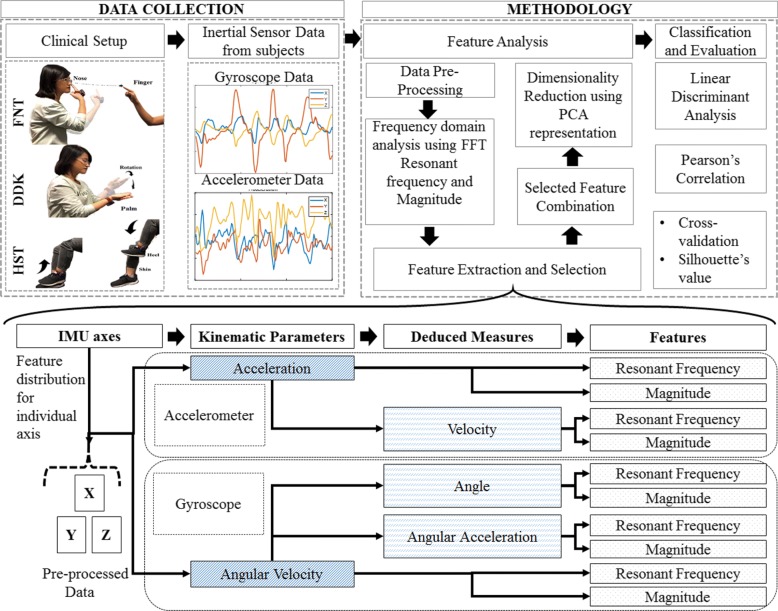
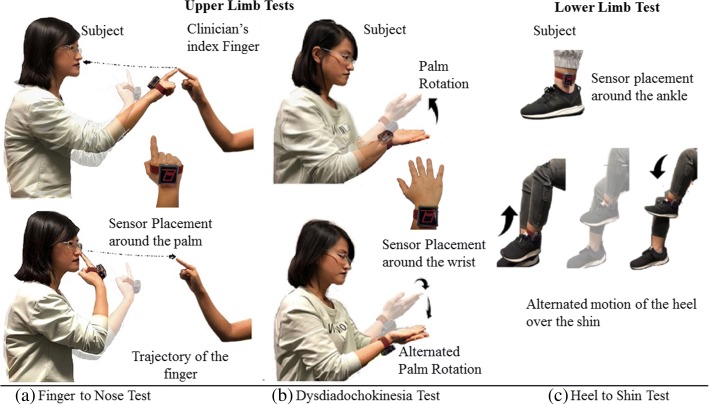
Background: Cerebellar damage can often result in disabilities affecting the peripheral regions of the body. These include poor and inaccurate coordination, tremors and irregular movements that often manifest as disorders associated with balance, gait and speech. The severity assessment of Cerebellar ataxia (CA) is determined by expert opinion and is likely to be subjective in nature. This paper investigates automated versions of three commonly used tests: Finger to Nose test (FNT), test for upper limb Dysdiadochokinesia Test (DDK) and Heel to Shin Test (HST), in evaluating disability due to CA.
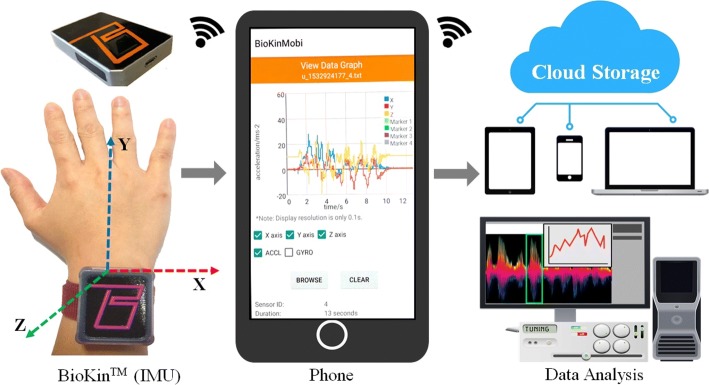
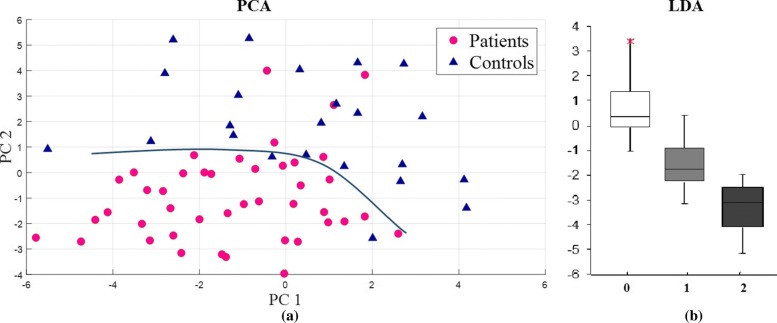
Methods: Limb movements associated with these tests are measured using Inertial Measurement Units (IMU) to capture the disability. Kinematic parameters such as acceleration, velocity and angle are considered in both time and frequency domain in three orthogonal axes to obtain relevant disability related information. The collective dominance in the data distributions of the underlying features were observed though the Principal Component Analysis (PCA). The dominant features were combined to substantiate the correlation with the expert clinical assessments through Linear Discriminant Analysis. Here, the Pearson correlation is used to examine the relationship between the objective assessments and the expert clinical scores while the performance was also verified by means of cross validation.
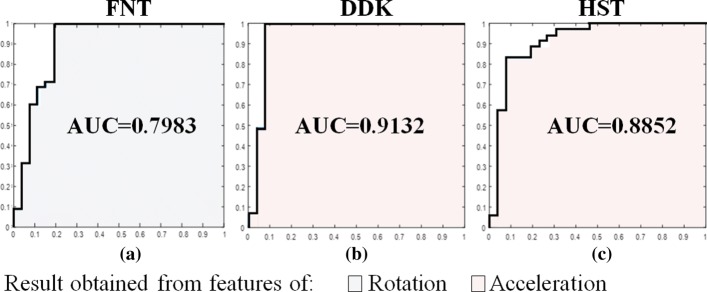
Results: The experimental results show that acceleration is a major feature in DDK and HST, whereas rotation is the main feature responsible for classification in FNT. Combining the features enhanced the correlations in each domain. The subject data was classified based on the severity information based on expert clinical scores.
Conclusion: For the predominantly translational movement in the upper limb FNT, the rotation captures disability and for the DDK test with predominantly rotational movements, the linear acceleration captures the disability but cannot be extended to the lower limb HST. The orthogonal direction manifestation of ataxia attributed to sensory measurements was determined for each test.
Trial registration: Human Research and Ethics Committee, Royal Victorian Eye and Ear Hospital, East Melbourne, Australia (HREC Reference Number: 11/994H/16).
Keywords: Diadochokinesia (DDK); Fast fourier transforms (FFT); Finger-to-nose (FNT); Heel shin test (HST); Principal component analysis (PCA).
Conflict of interest statement
Ethics approval and consent to participate
All the participants signed informed consent forms and the study was approved by the Human Research and Ethics Committee, Royal Victorian Eye and Ear Hospital, East Melbourne, Australia (HREC Reference Number: 11/994H/16).
Consent for publication
Written informed consent for publication was obtained from the subjects.
Competing interests
Pubudu N. Pathirana was involved in the initial design and development of
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures




References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
