

A multicenter study of body mass index in cancer patients treated with anti-PD-1/PD-L1 immune checkpoint inhibitors: when overweight becomes favorable
- PMID: 30813970
- PMCID: PMC6391761
- DOI: 10.1186/s40425-019-0527-y
A multicenter study of body mass index in cancer patients treated with anti-PD-1/PD-L1 immune checkpoint inhibitors: when overweight becomes favorable
Abstract
Background: Recent evidence suggested a potential correlation between overweight and the efficacy of immune checkpoint inhibitors (ICIs) in cancer patients.
Patients and methods: We conducted a retrospective study of advanced cancer patients consecutively treated with anti-PD-1/PD-L1 inhibitors, in order to compare clinical outcomes according to baseline BMI levels as primary analysis. Based on their BMI, patients were categorized into overweight/obese (≥ 25) and non-overweight (< 25). A gender analysis was also performed, using the same binomial cut-off. Further subgroup analyses were performed categorizing patients into underweight, normal weight, overweight and obese.
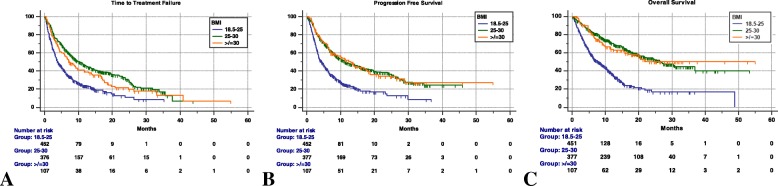
Results: Between September 2013 and May 2018, 976 patients were evaluated. The median age was 68 years, male/female ratio was 663/313. Primary tumors were: NSCLC (65.1%), melanoma (18.7%), renal cell carcinoma (13.8%) and others (2.4%). ECOG-PS was ≥2 in 145 patients (14.9%). PD-1/PD-L1 inhibitors were administered as first-line treatment in 26.6% of cases. Median BMI was 24.9: 492 patients (50.6%) were non-overweight, 480 patients (50.4%) were overweight/obese. 25.2% of non-overweight patients experienced irAEs of any grade, while 55.6% of overweight/obese patients (p < 0.0001). ORR was significantly higher in overweight/obese patients compared to non-overweight (p < 0.0001). Median follow-up was 17.2 months. Median TTF, PFS and OS were significantly longer for overweight/obese patients in univariate (p < 0.0001, for all the survival intervals) and multivariate models (p = 0.0009, p < 0.0001 and p < 0.0001 respectively). The significance was confirmed in both sex, except for PFS in male patients (p = 0.0668).
Conclusions: Overweight could be considered a tumorigenic immune-dysfunction that could be effectively reversed by ICIs. BMI could be a useful predictive tool in clinical practice and a stratification factor in prospective clinical trials with ICIs.
Keywords: Anti-PD-1/PD-L1; BMI; Cancer; Immunotherapy; Obesity; Overweight.
Conflict of interest statement
Ethics approval and consent to participate
All patients provided written, informed consent to treatment with immunotherapy. All patients alive at the time of data collection provided an informed consent for the present retrospective analysis. The procedures followed were in accordance with the precepts of Good Clinical Practice and the declaration of Helsinki. The study was approved by the respective local ethical committees on human experimentation of each institution, after previous approval by the coordinating center (University of L’Aquila, Internal Review Board protocol number 32865, approved on July 24th, 2018).
Consent for publication
Not applicable.
Competing interests
Dr Alessio Cortellini received grants as speaker by MSD, Astra-Zeneca and Boehringer Ingelheim, gran consultancies by BMS and Ipsen; dr Marcello Tiseo received grant as speaker and advisory role by Astra-Zeneca, Pfizer, Eli-Lilly, BMS, Novartis, Roche, MSD, Boehringer Ingelheim, Otsuka, Pierre Fabre; dr Maria Giuseppa Vitale received travel grants and speaker fees by BMS, Ipsen Astellas, Jansen, Novartis and Pfizer; dr Sebatiano Buti received grants as speaker and advisory role by BMS, Pfizer, MSD, Ipsen, Novartis, Astra-Zeneca; dr. Melissa Bersanelli received honoraria as speaker at scientific events and as consultant for advisory role by BMS and Pfizer.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials