

Neutrophil Dysfunction in the Airways of Children with Acute Respiratory Failure Due to Lower Respiratory Tract Viral and Bacterial Coinfections
- PMID: 30814584
- PMCID: PMC6393569
- DOI: 10.1038/s41598-019-39726-w
Neutrophil Dysfunction in the Airways of Children with Acute Respiratory Failure Due to Lower Respiratory Tract Viral and Bacterial Coinfections
Abstract
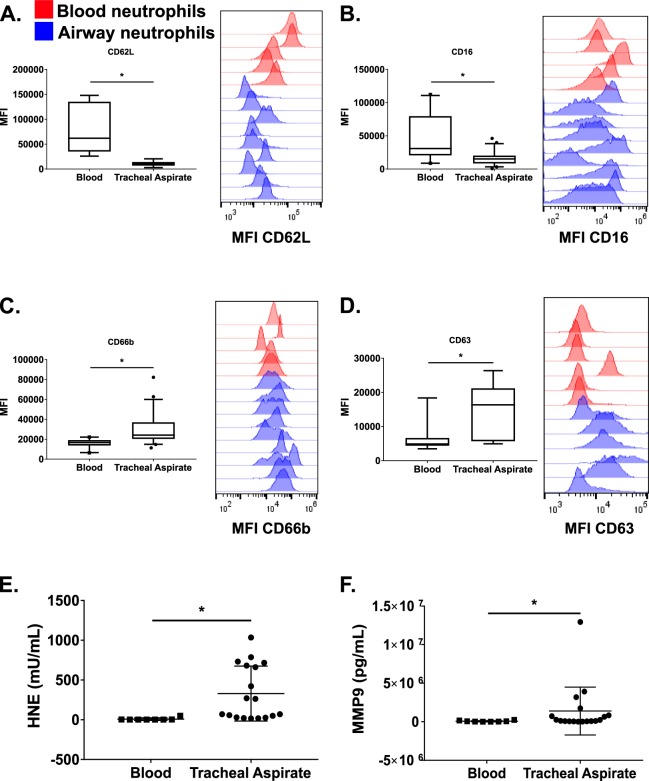
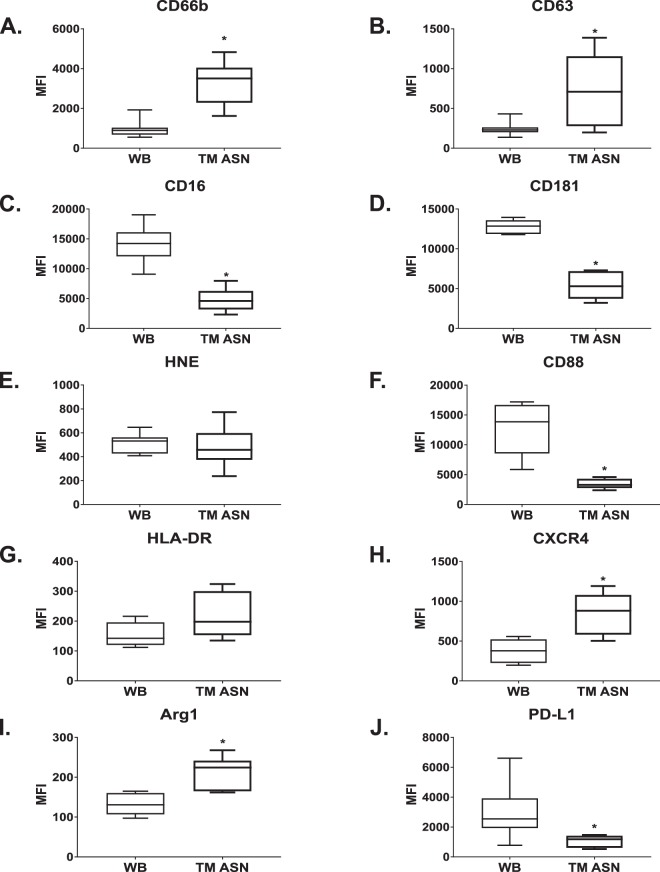
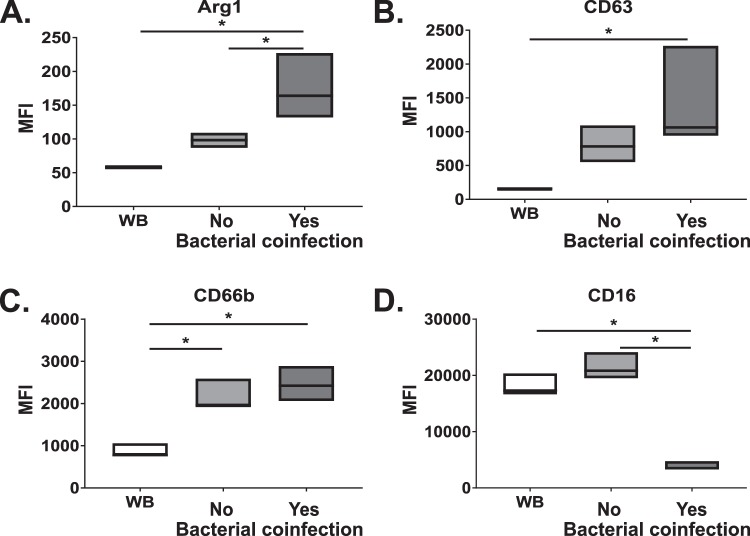
Neutrophils are recruited to the airways of patients with acute respiratory distress syndrome (ARDS) where they acquire an activated pro-survival phenotype with an enhanced respiratory burst thought to contribute to ARDS pathophysiology. Our in vitro model enables blood neutrophil transepithelial migration into cell-free tracheal aspirate fluid from patients to recapitulate the primary airway neutrophil phenotype observed in vivo. Neutrophils transmigrated through our model toward airway fluid from children with lower respiratory viral infections coinfected with bacteria had elevated levels of neutrophil activation markers but paradoxically exhibited an inability to kill bacteria and a defective respiratory burst compared with children without bacterial coinfection. The airway fluid from children with bacterial coinfections had higher levels of neutrophil elastase activity, as well as myeloperoxidase levels compared to children without bacterial coinfection. Neutrophils transmigrated into the aspirate fluid from children with bacterial coinfection showed decreased respiratory burst and killing activity against H. influenzae and S. aureus compared to those transmigrated into the aspirate fluid from children without bacterial coinfection. Use of a novel transmigration model recapitulates this pathological phenotype in vitro that would otherwise be impossible in a patient, opening avenues for future mechanistic and therapeutic research.
Conflict of interest statement
Drs. Grunwell, Fitzpatrick, and Tirouvanziam received support for research from the National Institutes of Health. None of the authors have any conflicts of interest. Dr. Grunwell is supported by the Atlanta Pediatric Scholars Program grant K12HD072245.
Figures




References
-
- Khemani RG, Smith LS, Zimmerman JJ, Erickson S ; Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome: definition, incidence, and epidemiology: proceedings from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med. 2015;16:S23–40. doi: 10.1097/PCC.0000000000000432. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
