

Fibroblast origin shapes tissue homeostasis, epidermal differentiation, and drug uptake
- PMID: 30814627
- PMCID: PMC6393472
- DOI: 10.1038/s41598-019-39770-6
Fibroblast origin shapes tissue homeostasis, epidermal differentiation, and drug uptake
Abstract
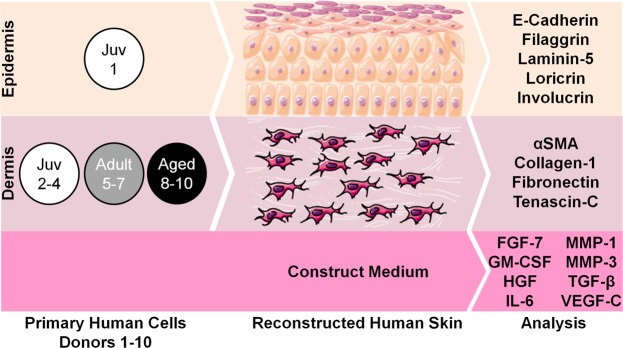
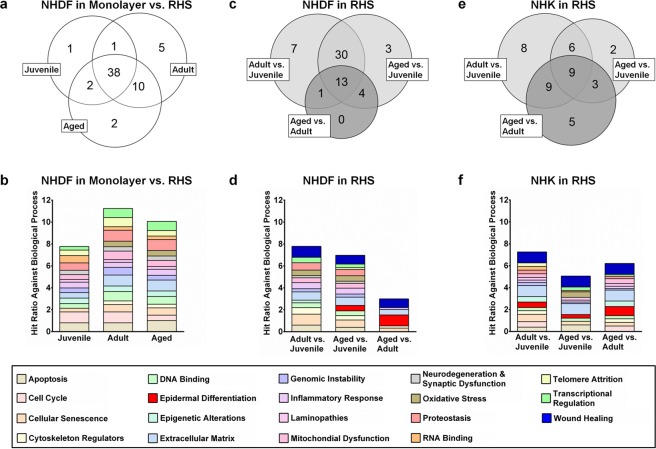
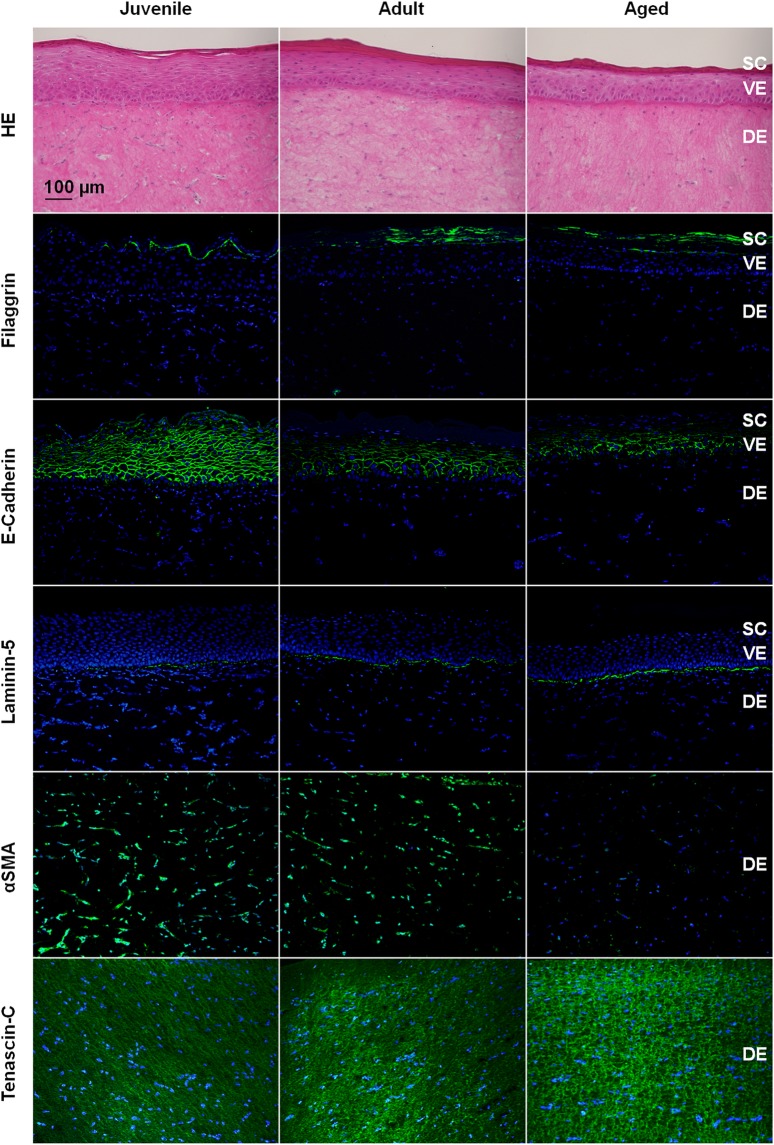
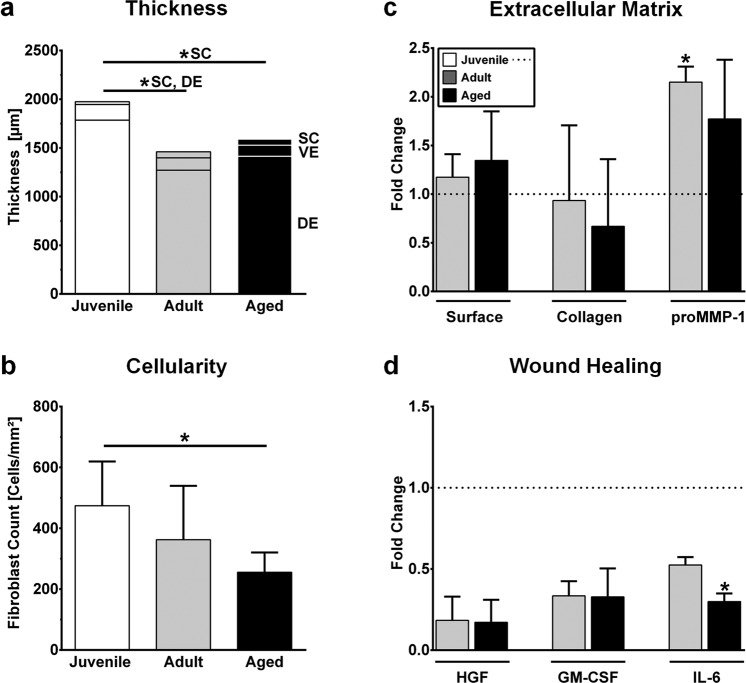
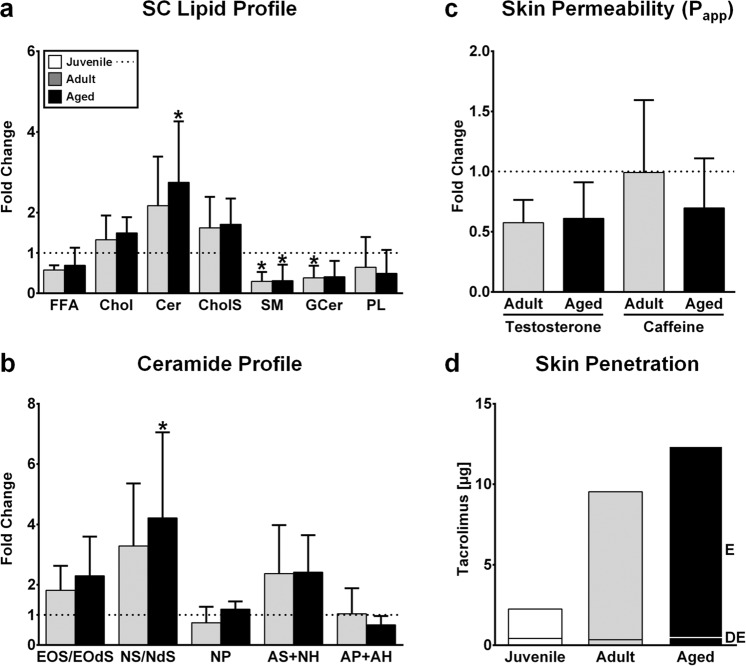
Preclinical studies frequently lack predictive value for human conditions. Human cell-based disease models that reflect patient heterogeneity may reduce the high failure rates of preclinical research. Herein, we investigated the impact of primary cell age and body region on skin homeostasis, epidermal differentiation, and drug uptake. Fibroblasts derived from the breast skin of female 20- to 30-year-olds or 60- to 70-year-olds and fibroblasts from juvenile foreskin (<10 years old) were compared in cell monolayers and in reconstructed human skin (RHS). RHS containing aged fibroblasts differed from its juvenile and adult counterparts, especially in terms of the dermal extracellular matrix composition and interleukin-6 levels. The site from which the fibroblasts were derived appeared to alter fibroblast-keratinocyte crosstalk by affecting, among other things, the levels of granulocyte-macrophage colony-stimulating factor. Consequently, the epidermal expression of filaggrin and e-cadherin was increased in RHS containing breast skin fibroblasts, as were lipid levels in the stratum corneum. In conclusion, the region of the body from which fibroblasts are derived appears to affect the epidermal differentiation of RHS, while the age of the fibroblast donors determines the expression of proteins involved in wound healing. Emulating patient heterogeneity in preclinical studies might improve the treatment of age-related skin conditions.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
