

Pre-hospital plasma in haemorrhagic shock management: current opinion and meta-analysis of randomized trials
- PMID: 30815028
- PMCID: PMC6377767
- DOI: 10.1186/s13017-019-0226-5
Pre-hospital plasma in haemorrhagic shock management: current opinion and meta-analysis of randomized trials
Abstract
Background: Trauma-induced coagulopathy is one of the most difficult issues to manage in severely injured patients. The plasma efficacy in treating haemorrhagic-shocked patients is well known. The debated issue is the timing at which it should be administered. Few evidences exist regarding the effects on mortality consequent to the use of plasma alone given in pre-hospital setting. Recently, two randomized trials reported interesting and discordant results. The present paper aims to analyse data from those two randomized trials in order to obtain more univocal results.
Methods: A systematic review with meta-analysis of randomized controlled trials (RCTs) of pre-hospital plasma vs. usual care in patients with haemorrhagic shock.
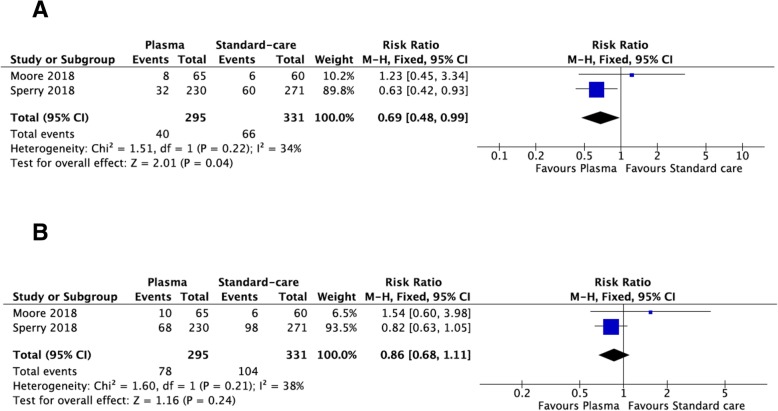
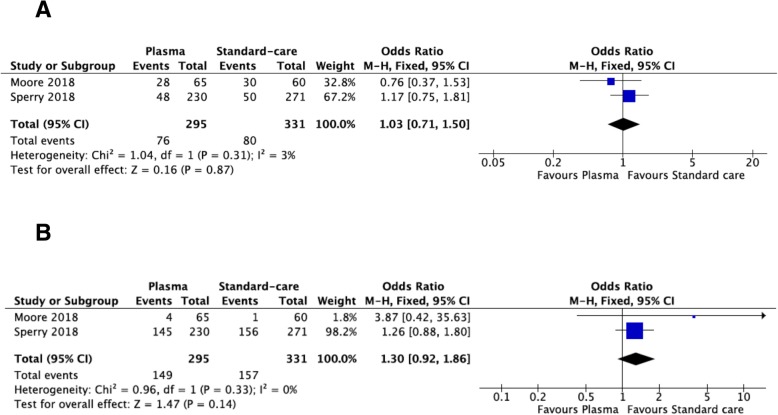
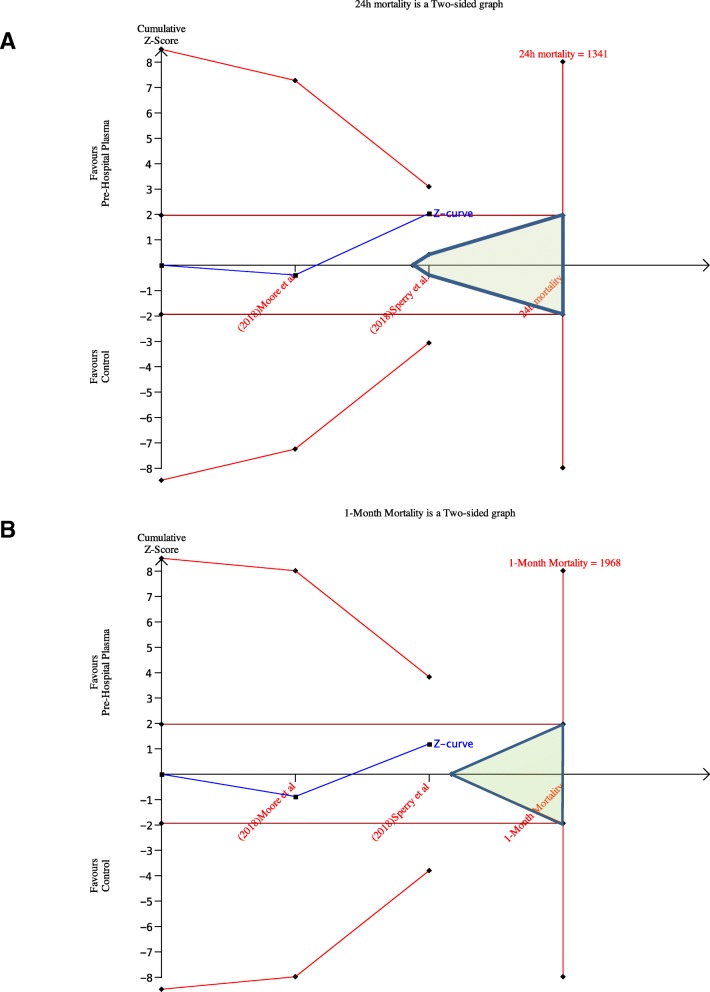
Results: Two high-quality RCTs have been included with 626 patients (295 in plasma and 331 in usual care arm). Twenty-four-hour mortality seems to be reduced in pre-hospital plasma group (RR = 0.69; 95% CI = 0.48-0.99). Pre-hospital plasma has no significant effect on 1-month mortality (RR = 0.86; 95% CI = 0.68-1.11) as on acute lung injury and on multi-organ failure rates (OR = 1.03; 95% CI = 0.71-1.50, and OR = 1.30; 95% CI = 0.92-1.86, respectively).
Conclusions: Pre-hospital plasma infusion seems to reduce 24-h mortality in haemorrhagic shock patients. It does not seem to influence 1-month mortality, acute lung injury and multi-organ failure rates.Level of evidence: Level IStudy type: Systematic review with Meta-analysis.
Keywords: Haemorrhagic; Management; Meta-analysis; Pre-hospital; Shock; Trauma; Treatment.
Conflict of interest statement
Not applicableNot applicableThe authors declare that they have no competing interests.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Brown JB, Cohen MJ, Minei JP, Maier RV, West MA, Billiar TR, Peitzman AB, Moore EE, Cushieri J, Inflammation SJL, Host response to injury I Debunking the survival bias myth: characterization of mortality during the initial 24 hours for patients requiring massive transfusion. J Trauma Acute Care Surg. 2012;73(2):358–364. doi: 10.1097/TA.0b013e31825889ba. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
