

Facial Fractures as a Result of Falls in the Elderly: Concomitant Injuries and Management Strategies
- PMID: 30815215
- PMCID: PMC6391279
- DOI: 10.1055/s-0038-1642034
Facial Fractures as a Result of Falls in the Elderly: Concomitant Injuries and Management Strategies
Abstract
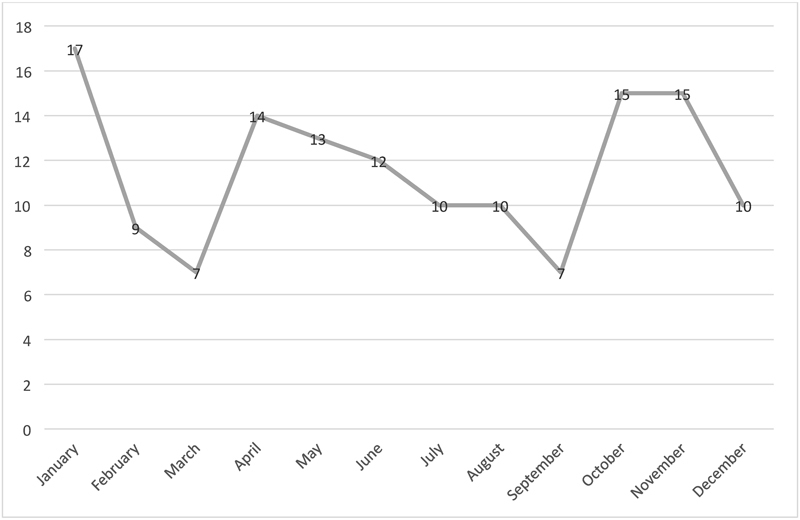
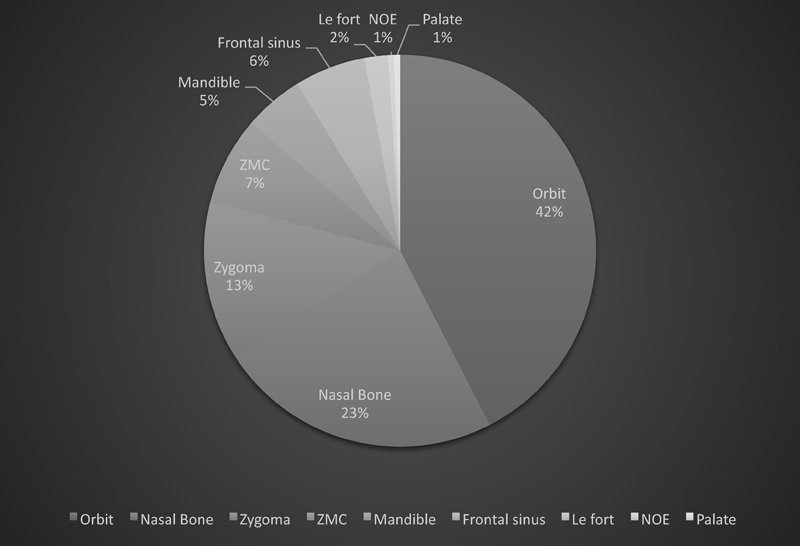
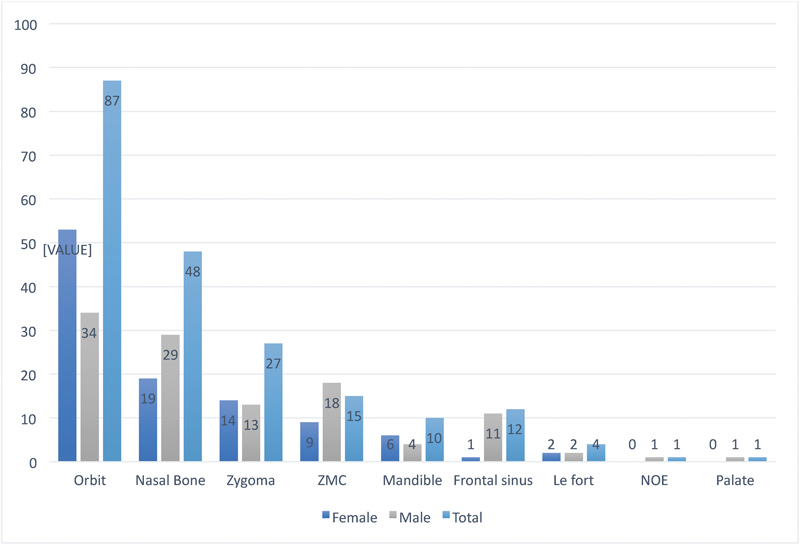
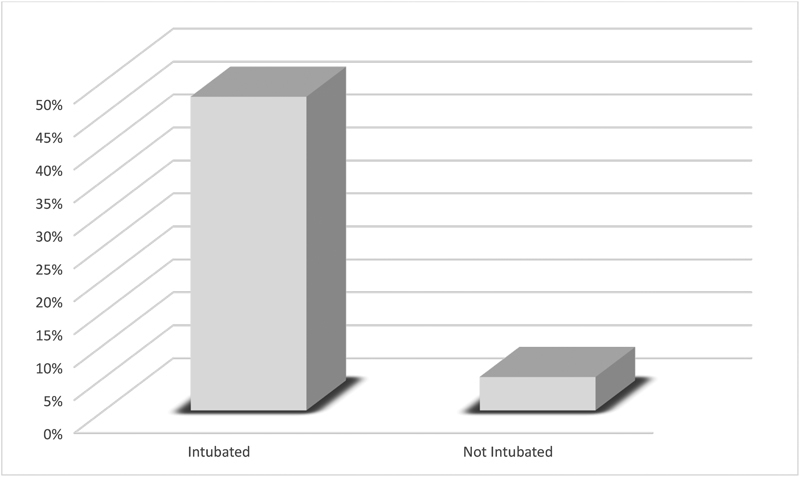
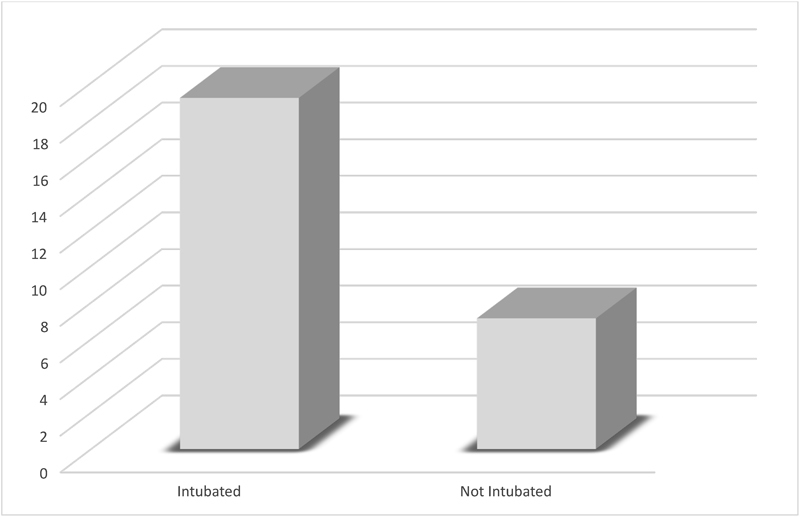
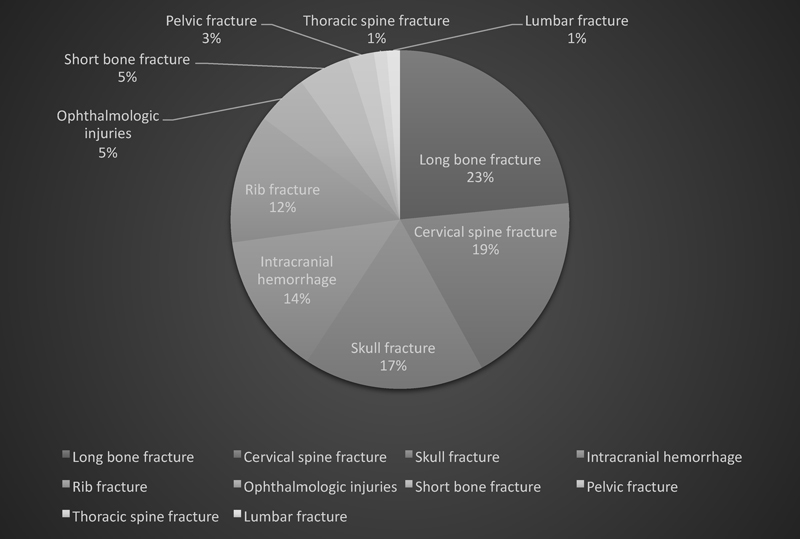
Mechanical falls are a common cause of facial trauma in the elderly population. It has been shown that the likelihood of sustaining a facial fracture due to a fall or activities of daily life significantly increases with age. Craniomaxillofacial fractures are most common during the first three decades of life; however, elderly patients more frequently require lengthy hospital stays and surgical intervention, and have shown increased complication rates compared with younger patients. The objective of this study was to examine the prevalence of facial fractures secondary to mechanical falls in the elderly population to analyze mechanism of injury, comorbidities, and fracture management. A retrospective review of all facial fractures as a result of falls in the elderly population in a level 1 trauma center in an urban environment was performed for the years 2002 to 2012. Patient demographics were collected, as well as location of fractures, concomitant injuries, and surgical management strategies. During the time period examined, 139 patients were identified as greater than 60 years of age and having sustained a fracture of the facial skeleton as the result of a fall. The average age was 75.7 (range, 60-103) years, with no gender predominance of 50.4% female and 49.6% male. There were a total of 205 fractures recorded. The most common fractures were those of the orbit (42.0%), nasal bone (23.4%), zygoma (13.2%), and zygomaticomaxillary complex (7.32%). The average Glasgow Coma Scale on arrival was 12.8 (range, 3-15). Uncontrolled hemorrhage was noted on presentation to the trauma bay in five patients. Twenty-one patients were intubated on, or prior to, arrival to the trauma bay, and 44 required a surgical airway. The most common concomitant injury was a long bone fracture (23.5%), followed by cervical spine fracture (18.5%), skull fracture (17.3%), intracerebral hemorrhage (17.3%), rib fracture (17.3%), ophthalmologic injuries (6.2%), short bone fracture (4.9%), pelvic fracture (2.9%), thoracic spine fracture (1.2%), and lumbar spine fracture (1.2%). Of the 114 patients admitted to the hospital, 53 were admitted to an intensive care setting. The average hospital length of stay was 8.97 days (range, 0-125). Sixteen patients expired. Surgical management of fractures in the operating room was required in 47 of the 139 patients. Of the patients treated, 36.2% required an open reduction and internal fixation procedure. Facial fractures as a result of falls in the geriatric population represent an increasing number of cases in clinical practice as life expectancy steadily rises. These patients require a specific standard of treatment since they are more susceptible to nosocomial infections, as well as have higher complication rates and longer recovery time. Concomitant injuries such as cervical spine and pelvic fractures can greatly increase risk of mortality. Surgical and soft tissue management must be approached with caution to optimize function and aesthetics while preventing secondary infection. The authors hope that this study can provide some insight and further investigation as there is a dearth of literature to the management of facial fractures in falls in elderly patients.
Keywords: elderly facial fractures; elderly falls; facial trauma in the elderly; falls in the elderly.
Conflict of interest statement
Figures
Similar articles
-
Examination of life-threatening injuries in 431 pediatric facial fractures at a level 1 trauma center.J Craniofac Surg. 2014 Sep;25(5):1825-8. doi: 10.1097/SCS.0000000000001055. J Craniofac Surg. 2014. PMID: 25203578
-
Pediatric Pedestrian Facial Fracture Patterns and Management Following Motor Vehicle Collisions.J Craniofac Surg. 2020 Jan/Feb;31(1):265-268. doi: 10.1097/SCS.0000000000006034. J Craniofac Surg. 2020. PMID: 31821213
-
Traumatic Falls in the Pediatric Population: Facial Fracture Patterns Observed in a Leading Cause of Childhood Injury.Ann Plast Surg. 2019 Apr;82(4S Suppl 3):S195-S198. doi: 10.1097/SAP.0000000000001861. Ann Plast Surg. 2019. PMID: 30730318
-
A Review of Frontal Orbital and Frontal Sinus Fractures and Associated Ocular Injuries - Level I Trauma Center - University Hospital Experience.J Craniofac Surg. 2021 Jun 1;32(4):1615-1618. doi: 10.1097/SCS.0000000000007422. J Craniofac Surg. 2021. PMID: 33741886 Review.
-
Maxillofacial trauma in central karnataka, India: an outcome of 95 cases in a regional trauma care centre.Craniomaxillofac Trauma Reconstr. 2012 Dec;5(4):197-204. doi: 10.1055/s-0032-1322536. Epub 2012 Jul 31. Craniomaxillofac Trauma Reconstr. 2012. PMID: 24294402 Free PMC article. Review.
Cited by
-
Single institutional experience of geriatric maxillofacial trauma patients: a retrospective study.J Korean Assoc Oral Maxillofac Surg. 2025 Apr 30;51(2):102-107. doi: 10.5125/jkaoms.2025.51.2.102. J Korean Assoc Oral Maxillofac Surg. 2025. PMID: 40296734 Free PMC article.
-
Patterns of Midface and Mandible Fractures in a Government Hospital.Craniomaxillofac Trauma Reconstr. 2024 Sep;17(3):194-202. doi: 10.1177/19433875231151317. Epub 2023 Jan 19. Craniomaxillofac Trauma Reconstr. 2024. PMID: 39329076 Free PMC article.
-
Emergency versus semi-elective management of mandible fractures: a Maxillofacial Trainee Research Collaborative (MTReC) study.Ann R Coll Surg Engl. 2023 May;105(5):461-468. doi: 10.1308/rcsann.2022.0063. Epub 2022 Jul 29. Ann R Coll Surg Engl. 2023. PMID: 35904336 Free PMC article.
-
Trends in the incidence, prevalence and years lived with disability of facial fracture at global, regional and national levels from 1990 to 2017.PeerJ. 2021 Jan 19;9:e10693. doi: 10.7717/peerj.10693. eCollection 2021. PeerJ. 2021. PMID: 33552726 Free PMC article.
-
The epidemiology of alcohol involved facial injuries.Oral Maxillofac Surg. 2025 Jan 28;29(1):47. doi: 10.1007/s10006-025-01343-5. Oral Maxillofac Surg. 2025. PMID: 39873853 Free PMC article.
References
-
- Ortman J M, Velkoff V A, Hogan H. Suitland, MD: US Census Bureau; 2014. An Aging Nation: The Older Population in the United States. Report number P25-1140.
-
- National Center for Health Statistics.Health, United States, 2016: With Chartbook on Long-term Trends in Health Hyattsville, MD: 2017 - PubMed
-
- Wong C A, Recktenwald A J, Jones M L, Waterman B M, Bollini M L, Dunagan W C. The cost of serious fall-related injuries at three Midwestern hospitals. Jt Comm J Qual Patient Saf. 2011;37(02):81–87. - PubMed
-
- Schwab C W, Kauder D R. Trauma in the geriatric patient. Arch Surg. 1992;127(06):701–706. - PubMed
LinkOut - more resources
Full Text Sources