

Challenges in the diagnosis and treatment of gestational trophoblastic neoplasia worldwide
- PMID: 30815369
- PMCID: PMC6390119
- DOI: 10.5306/wjco.v10.i2.28
Challenges in the diagnosis and treatment of gestational trophoblastic neoplasia worldwide
Abstract
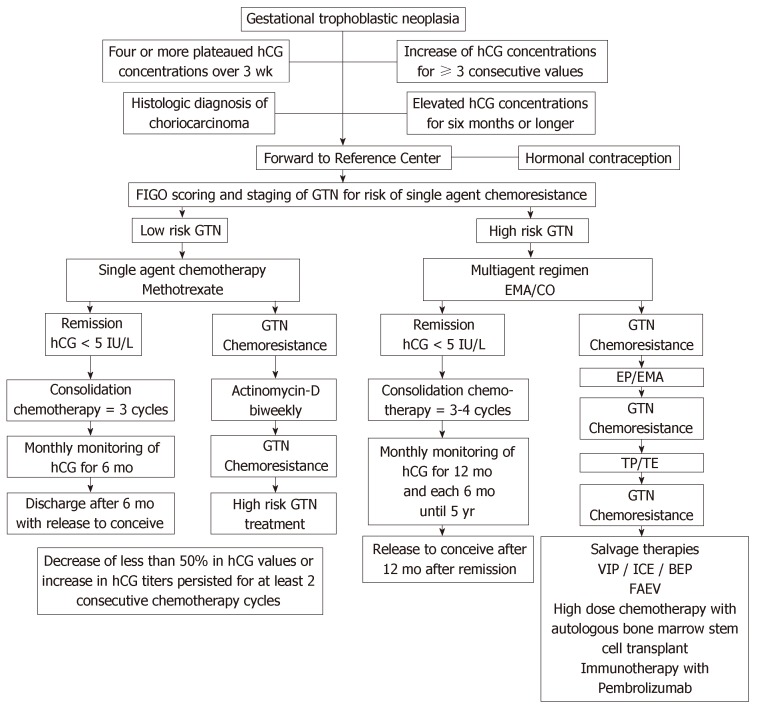
Gestational trophoblastic neoplasia (GTN) is a rare tumor that originates from pregnancy that includes invasive mole, choriocarcinoma (CCA), placental site trophoblastic tumor and epithelioid trophoblastic tumor (PSTT/ETT). GTN presents different degrees of proliferation, invasion and dissemination, but, if treated in reference centers, has high cure rates, even in multi-metastatic cases. The diagnosis of GTN following a hydatidiform molar pregnancy is made according to the International Federation of Gynecology and Obstetrics (FIGO) 2000 criteria: four or more plateaued human chorionic gonadotropin (hCG) concentrations over three weeks; rise in hCG for three consecutive weekly measurements over at least a period of 2 weeks or more; and an elevated but falling hCG concentrations six or more months after molar evacuation. However, the latter reason for treatment is no longer used by many centers. In addition, GTN is diagnosed with a pathological diagnosis of CCA or PSTT/ETT. For staging after a molar pregnancy, FIGO recommends pelvic-transvaginal Doppler ultrasound and chest X-ray. In cases of pulmonary metastases with more than 1 cm, the screening should be complemented with chest computed tomography and brain magnetic resonance image. Single agent chemotherapy, usually Methotrexate (MTX) or Actinomycin-D (Act-D), can cure about 70% of patients with FIGO/World Health Organization (WHO) prognosis risk score ≤ 6 (low risk), reserving multiple agent chemotherapy, such as EMA/CO (Etoposide, MTX, Act-D, Cyclophosphamide and Oncovin) for cases with FIGO/WHO prognosis risk score ≥ 7 (high risk) that is often metastatic. Best overall cure rates for low and high risk disease is close to 100% and > 95%, respectively. The management of PSTT/ETT differs and cure rates tend to be a bit lower. The early diagnosis of this disease and the appropriate treatment avoid maternal death, allow the healing and maintenance of the reproductive potential of these women.
Keywords: Chemotherapy; Choriocarcinoma; Chorionic gonadotropin; Epithelioid trophoblastic tumor; Gestational trophoblastic neoplasia; Invasive mole; Placental site trophoblastic tumor.
Conflict of interest statement
Conflict-of-interest statement: The authors have no conflict of interest to declare.
Figures
References
-
- Biscaro A, Braga A, Berkowitz RS. Diagnosis, classification and treatment of gestational trophoblastic neoplasia. Rev Bras Ginecol Obstet. 2015;37:42–51. - PubMed
-
- Maestá I, Braga A. [Challenges of the treatment of patients with gestational trophoblastic disease] Rev Bras Ginecol Obstet. 2012;34:143–146. - PubMed
-
- Seckl MJ, Sebire NJ, Fisher RA, Golfier F, Massuger L, Sessa C ESMO Guidelines Working Group. Gestational trophoblastic disease: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24 Suppl 6:vi39–vi50. - PubMed
-
- Mangili G, Lorusso D, Brown J, Pfisterer J, Massuger L, Vaughan M, Ngan HY, Golfier F, Sekharan PK, Charry RC, Poveda A, Kim JW, Xiang Y, Berkowtiz R, Seckl MJ. Trophoblastic disease review for diagnosis and management: a joint report from the International Society for the Study of Trophoblastic Disease, European Organisation for the Treatment of Trophoblastic Disease, and the Gynecologic Cancer InterGroup. Int J Gynecol Cancer. 2014;24:S109–S116. - PubMed
-
- Hertz R, Li MC, Spencer DB. Effect of methotrexate therapy upon choriocarcinoma and chorioadenoma. Proc Soc Exp Biol Med. 1956;93:361–366. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
