

Extended resuscitative endovascular balloon occlusion of the aorta (REBOA)-induced type 2 myocardial ischemia: a time-dependent penalty
- PMID: 30815536
- PMCID: PMC6361364
- DOI: 10.1136/tsaco-2018-000194
Extended resuscitative endovascular balloon occlusion of the aorta (REBOA)-induced type 2 myocardial ischemia: a time-dependent penalty
Abstract
Background: Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) increases cardiac-afterload and is used for patients in hemorrhagic shock. The cardiac tolerance of prolonged afterload augmentation in this context is unknown. The aim of this study is to quantify cardiac injury, if any, following 2, 3 and 4 hours of REBOA.
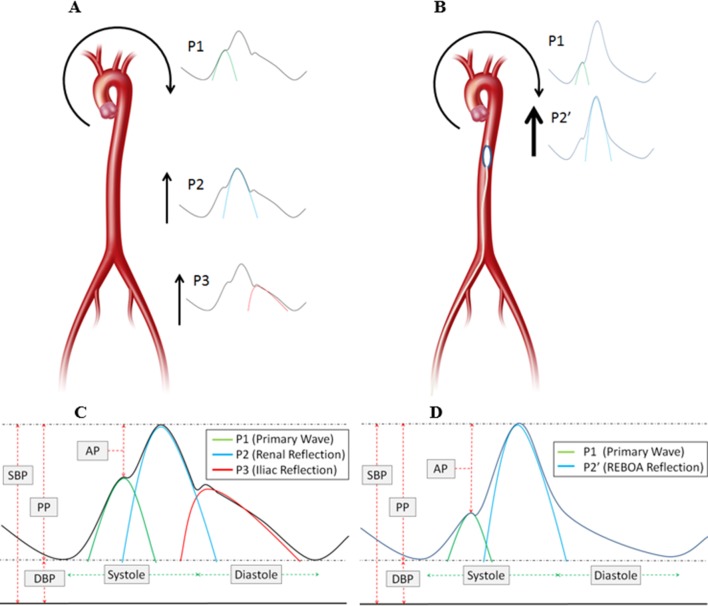
Methods: Anesthetized swine (70-90 kg) underwent a 40% controlled hemorrhage, followed by supraceliac resuscitative endovascular balloon occlusion of the aorta (REBOA) for 2 (n=5), 3 (n=5), and 4 hours (n=5). High-fidelity arterial wave form data were collected, and signal processing techniques were used to extract key inflection points. The adjusted augmentation index (AIx@75; augmentation pressure/pulse pressure, normalized for heart rate) was derived for use as a measure of aortic compliance (higher ratio = less compliance). Endpoints consisted of electrocardiographic, biochemical, and histologic markers of myocardial injury/ischemia. Regression modeling was used to assess the trend against time.
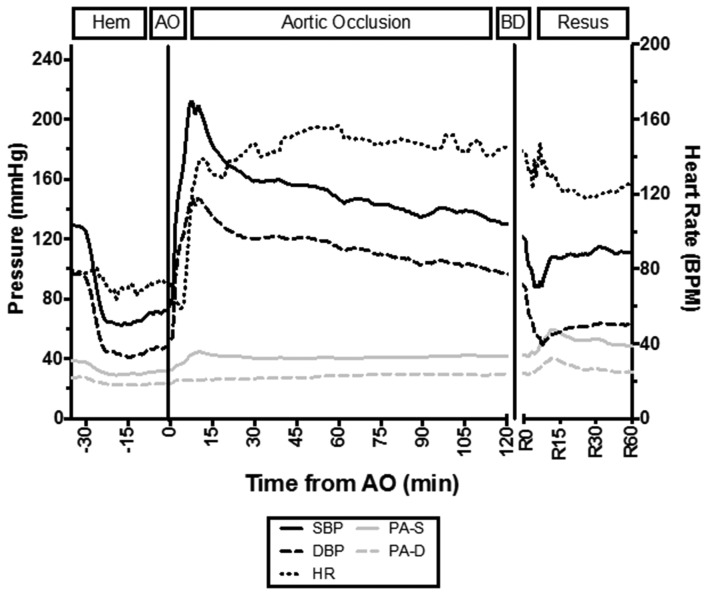
Results: All animals tolerated instrumentation, hemorrhage, and REBOA. The mean (±SD) systolic blood pressure (mm Hg) increased from 65±11 to 212±39 (p<0.001) during REBOA. The AIx@75 was significantly higher during REBOA than baseline, hemorrhage, and resuscitation phases (p<0.05). A time-dependent rise in troponin (R2=0.95; p<0.001) and T-wave deflection (R2=0.64; p<0.001) was observed. The maximum mean troponin (ng/mL) occurred at 4 hours (14.6±15.4) and maximum T-wave deflection (mm) at 65 minutes (3.0±1.8). All animals demonstrated histologic evidence of acute injury with increasing degrees of cellular myocardial injury.
Discussion: Prolonged REBOA may result in type 2 myocardial ischemia, which is time-dependent. This has important implications for patients where prolonged REBOA may be considered beneficial, and strategies to mitigate this effect require further investigation.
Level of evidence: II.
Keywords: aortic occlusion; arterial waveform; cardiac; cardiac injury; hemorrhage; ischemia; reboa; resuscitative endovascular balloon occlusion of the aorta.
Conflict of interest statement
Competing interests: JM is a clinical advisory board member for Prytime Medical.
Figures



Similar articles
-
Endovascular variable aortic control (EVAC) versus resuscitative endovascular balloon occlusion of the aorta (REBOA) in a swine model of hemorrhage and ischemia reperfusion injury.J Trauma Acute Care Surg. 2018 Sep;85(3):519-526. doi: 10.1097/TA.0000000000002008. J Trauma Acute Care Surg. 2018. PMID: 30142105
-
Extending the golden hour for Zone 1 resuscitative endovascular balloon occlusion of the aorta: Improved survival and reperfusion injury with intermittent versus continuous resuscitative endovascular balloon occlusion of the aorta of the aorta in a porcine severe truncal hemorrhage model.J Trauma Acute Care Surg. 2018 Aug;85(2):318-326. doi: 10.1097/TA.0000000000001964. J Trauma Acute Care Surg. 2018. PMID: 30080780
-
Resuscitative endovascular balloon occlusion of the aorta induced myocardial injury is mitigated by endovascular variable aortic control.J Trauma Acute Care Surg. 2019 Sep;87(3):590-598. doi: 10.1097/TA.0000000000002363. J Trauma Acute Care Surg. 2019. PMID: 31145381
-
Resuscitative Endovascular Balloon Occlusion of the Aorta (REBOA) Use in Animal Trauma Models.J Surg Res. 2021 Dec;268:125-135. doi: 10.1016/j.jss.2021.06.052. Epub 2021 Jul 23. J Surg Res. 2021. PMID: 34304008 Review.
-
Resuscitative Endovascular Balloon Occlusion of the Aorta: A Review for Emergency Clinicians.J Emerg Med. 2019 Jun;56(6):687-697. doi: 10.1016/j.jemermed.2019.03.030. Epub 2019 Apr 19. J Emerg Med. 2019. PMID: 31010604 Review.
Cited by
-
The Underlying Cardiovascular Mechanisms of Resuscitation and Injury of REBOA and Partial REBOA.Front Physiol. 2022 May 9;13:871073. doi: 10.3389/fphys.2022.871073. eCollection 2022. Front Physiol. 2022. PMID: 35615678 Free PMC article.
-
Intermittent thoracic resuscitative endovascular balloon occlusion of the aorta improves renal function compared to 60 min continuous application after porcine class III hemorrhage.Eur J Trauma Emerg Surg. 2023 Jun;49(3):1303-1313. doi: 10.1007/s00068-022-02189-2. Epub 2022 Dec 5. Eur J Trauma Emerg Surg. 2023. PMID: 36471055 Free PMC article.
-
Intra-aortic and Intra-caval Balloon Pump Devices in Experimental Non-traumatic Cardiac Arrest and Cardiopulmonary Resuscitation.J Cardiovasc Transl Res. 2023 Aug;16(4):948-955. doi: 10.1007/s12265-022-10343-9. Epub 2022 Dec 8. J Cardiovasc Transl Res. 2023. PMID: 36481982 Free PMC article.
-
Combined effect of intermittent hemostasis and a modified external hemorrhage control device in a lethal swine model.Heliyon. 2024 Aug 30;10(17):e37017. doi: 10.1016/j.heliyon.2024.e37017. eCollection 2024 Sep 15. Heliyon. 2024. PMID: 39296135 Free PMC article.
-
Complications associated with the use of resuscitative endovascular balloon occlusion of the aorta (REBOA): an updated review.Trauma Surg Acute Care Open. 2024 Feb 7;9(1):e001267. doi: 10.1136/tsaco-2023-001267. eCollection 2024. Trauma Surg Acute Care Open. 2024. PMID: 38347890 Free PMC article. Review.
References
-
- Wasicek PJ, Shanmuganathan K, Teeter WA, Gamble WB, Hu P, Stein DM, Scalea TM, Brenner ML. Assessment of blood flow patterns distal to aortic occlusion using CT in patients with resuscitative endovascular balloon occlusion of the aorta. J Am Coll Surg 2018;226:294–308. 10.1016/j.jamcollsurg.2017.12.005 - DOI - PubMed
-
- Manley JD, Mitchell BJ, DuBose JJ, Rasmussen TE. A modern case series of resuscitative endovascular balloon occlusion of the aorta (REBOA) in an out-of-hospital, combat casualty care setting. J Spec Oper Med 2017;17:1–8. - PubMed
-
- Sadek S, Lockey DJ, Lendrum RA, Perkins Z, Price J, Davies GE. Resuscitative endovascular balloon occlusion of the aorta (REBOA) in the pre-hospital setting: an additional resuscitation option for uncontrolled catastrophic haemorrhage. Resuscitation 2016;107:135–8. 10.1016/j.resuscitation.2016.06.029 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Research Materials