

Clinical Pharmacokinetics and Pharmacodynamics of Immune Checkpoint Inhibitors
- PMID: 30815848
- PMCID: PMC6584248
- DOI: 10.1007/s40262-019-00748-2
Clinical Pharmacokinetics and Pharmacodynamics of Immune Checkpoint Inhibitors
Abstract
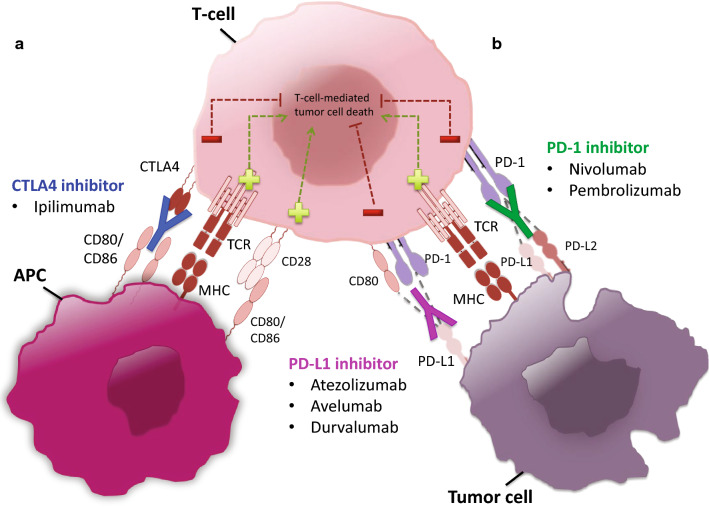
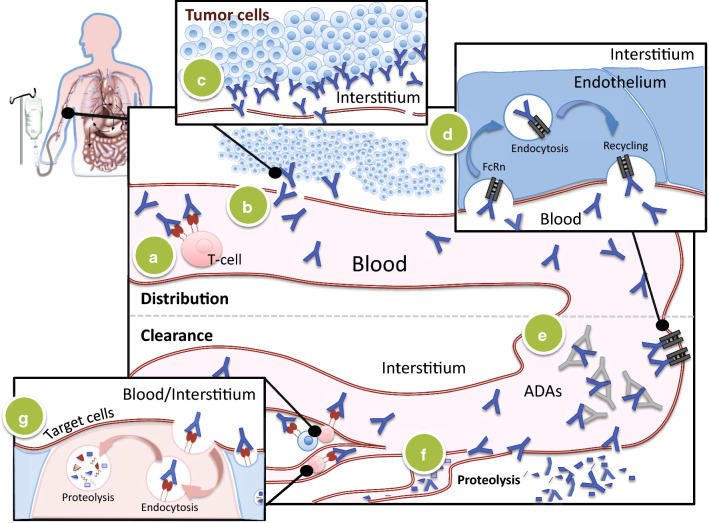
Immune checkpoint inhibitors (ICIs) have demonstrated significant clinical impact in improving overall survival of several malignancies associated with poor outcomes; however, only 20-40% of patients will show long-lasting survival. Further clarification of factors related to treatment response can support improvements in clinical outcome and guide the development of novel immune checkpoint therapies. In this article, we have provided an overview of the pharmacokinetic (PK) aspects related to current ICIs, which include target-mediated drug disposition and time-varying drug clearance. In response to the variation in treatment exposure of ICIs and the significant healthcare costs associated with these agents, arguments for both dose individualization and generalization are provided. We address important issues related to the efficacy and safety, the pharmacodynamics (PD), of ICIs, including exposure-response relationships related to clinical outcome. The unique PK and PD aspects of ICIs give rise to issues of confounding and suboptimal surrogate endpoints that complicate interpretation of exposure-response analysis. Biomarkers to identify patients benefiting from treatment with ICIs have been brought forward. However, validated biomarkers to monitor treatment response are currently lacking.
Conflict of interest statement
Maddalena Centanni, Dirk Jan A. R. Moes, Iñaki F. Trocóniz, Joseph Ciccolini, and Johan G. Coen van Hasselt have no conflicts of interest to declare related to the contents of this manuscript.
Figures
References
-
- Caroline R, Luc T, Igor B, Steven O, Jeffrey W, Claus G, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364:2517–2526. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
