

Migrated T lymphocytes into malignant pleural effusions: an indicator of good prognosis in lung adenocarcinoma patients
- PMID: 30816121
- PMCID: PMC6395746
- DOI: 10.1038/s41598-018-35840-3
Migrated T lymphocytes into malignant pleural effusions: an indicator of good prognosis in lung adenocarcinoma patients
Abstract
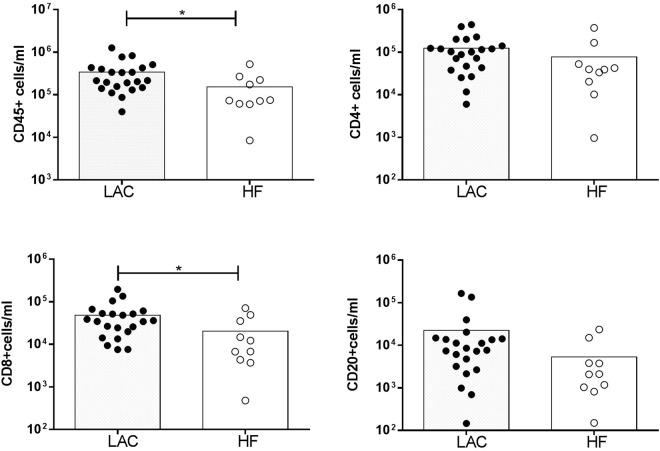
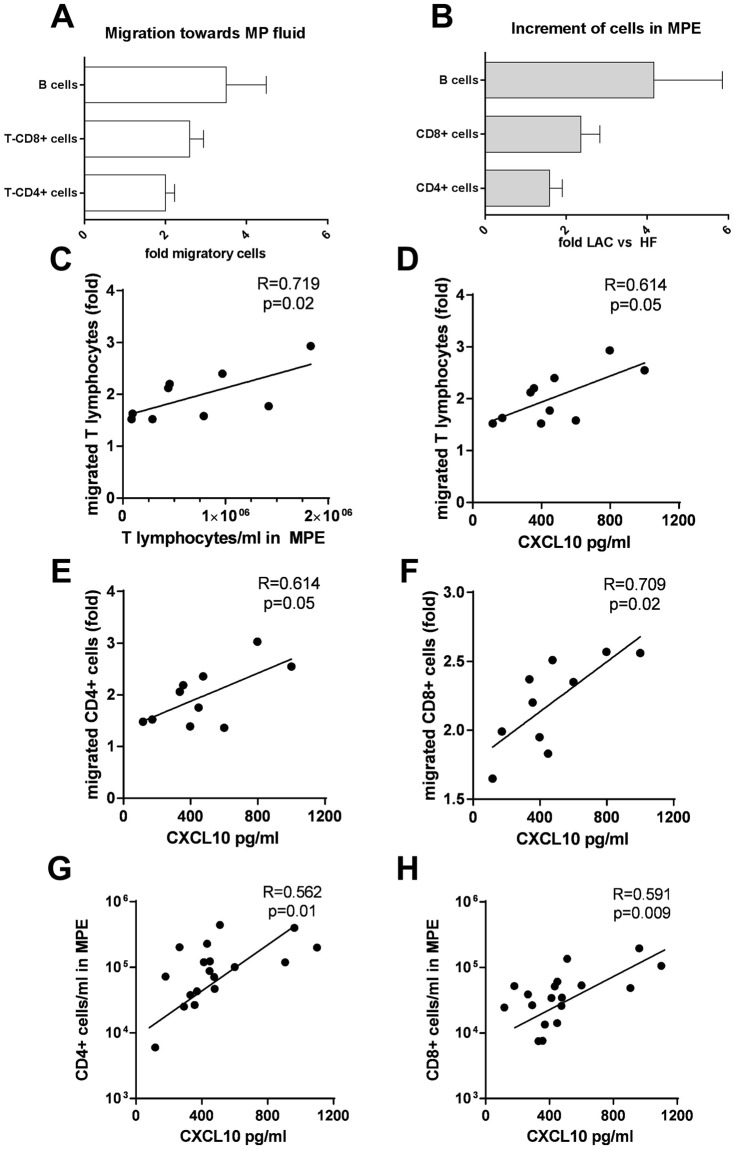
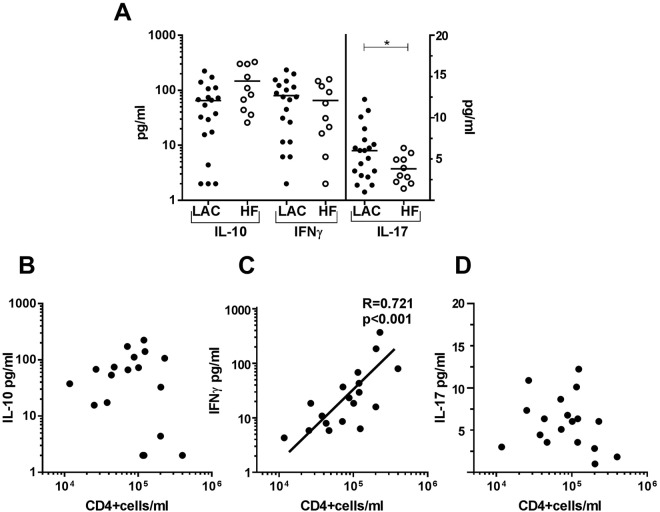
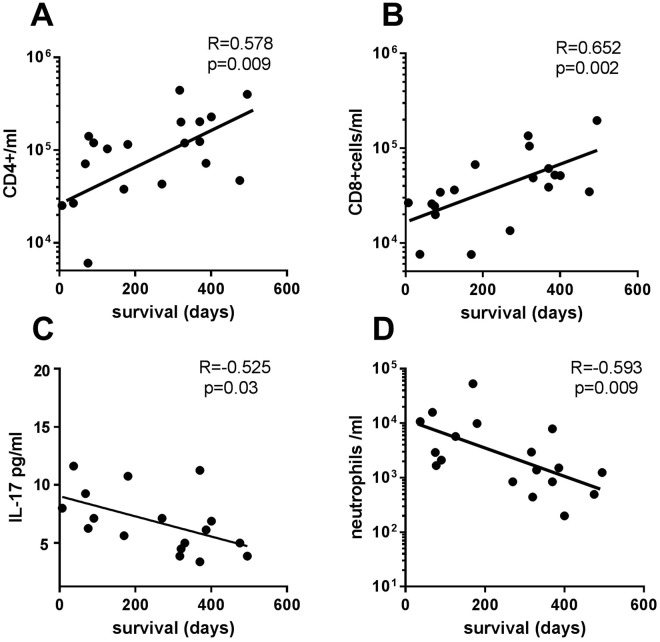
The presence of leukocyte subpopulations in malignant pleural effusions (MPEs) can have a different impact on tumor cell proliferation and vascular leakiness, their analysis can help to understand the metastatic microenvironment. We analyzed the relationship between the leukocyte subpopulation counts per ml of pleural fluid and the tumor cell count, molecular phenotype of lung adenocarcinoma (LAC), time from cancer diagnosis and previous oncologic therapy. We also evaluated the leukocyte composition of MPEs as a biomarker of prognosis. We determined CD4+ T, CD8+ T and CD20+ B cells, monocytes and neutrophils per ml in pleural effusions of 22 LAC and 10 heart failure (HF) patients by flow cytometry. Tumor cells were identified by morphology and CD326 expression. IFNγ, IL-10 and IL-17, and chemokines were determined by ELISAs and migratory response to pleural fluids by transwell assays. MPEs from LAC patients had more CD8+ T lymphocytes and a tendency to more CD4+ T and CD20+ B lymphocytes than HF-related fluids. However, no correlation was found between lymphocytes and tumor cells. In those MPEs which were detected >1 month from LAC diagnosis, there was a negative correlation between pleural tumor cells and CD8+ T lymphocytes. CXCL10 was responsible for the attraction of CD20+ B, CD4+ T and CD8+ T lymphocytes in malignant fluids. Concentrations of IL-17 were higher in MPEs than in HF-related effusions. Survival after MPE diagnosis correlated positively with CD4+ T and CD8+ T lymphocytes, but negatively with neutrophils and IL-17 levels. In conclusion, lymphocyte enrichment in MPEs from LAC patients is mostly due to local migration and increases patient survival.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
