

Factors Associated with Diabetes-Related Clinical Inertia in a Managed Care Population and Its Effect on Hemoglobin A1c Goal Attainment: A Claims-Based Analysis
- PMID: 30816810
- PMCID: PMC10397755
- DOI: 10.18553/jmcp.2019.25.3.304
Factors Associated with Diabetes-Related Clinical Inertia in a Managed Care Population and Its Effect on Hemoglobin A1c Goal Attainment: A Claims-Based Analysis
Abstract
Background: Despite evidence showing the benefits of treatment intensification following an elevated hemoglobin A1c (A1c), clinical inertia, or failure to establish and/or escalate treatment to achieve treatment goals, is a concern among patients diagnosed with type 2 diabetes (T2DM). Clinical inertia may contribute to increased health care utilization and costs due to poor clinical outcomes in MCOs.
Objectives: To (a) identify factors associated with clinical inertia in T2DM and (b) determine differences in A1c goal attainment between patients who experience clinical inertia versus treatment intensification in a commercially insured population.
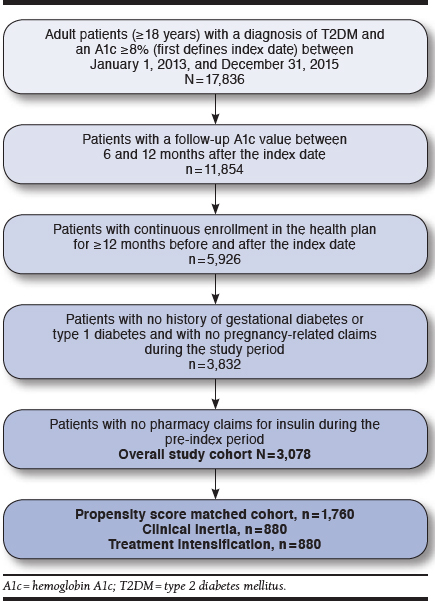
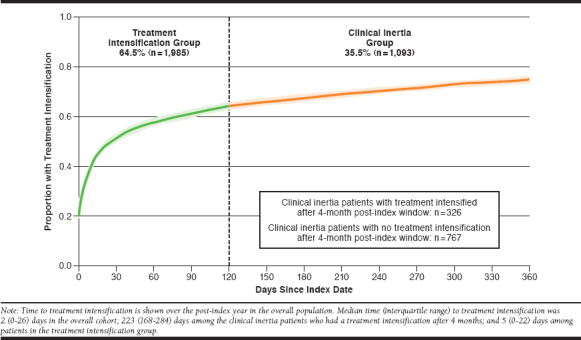
Methods: Medical and pharmacy claims data were used to identify commercially insured patients in a regional MCO with a recorded A1c ≥ 8.0% between January 1, 2013, and December 31, 2015. In the 4 months following the first elevated A1c value (index date), patients were classified into 2 groups: treatment intensification or clinical inertia. Treatment intensification was defined as the addition of ≥ 1 new noninsulin antihyperglycemic medication, the addition of insulin, or a dose increase of any current noninsulin antihyperglycemic medication. Patients were required to have ≥ 1 follow-up A1c value 6-12 months after the index date and continuous enrollment in the health plan for 12 months before and after the index date. Patients were excluded if they had a diagnosis for gestational diabetes or type 1 diabetes or if they were on insulin in the pre-index period. The primary outcome of attaining A1c < 7.0% was compared between groups after propensity score matching (PSM). Factors associated with clinical inertia were identified using logistic regression.
Results: 3,078 patients, with a mean (SD) age of 54.4 (10.6) years and a mean (SD) baseline A1c of 9.6% (1.7), were included in the study. Of these, 1,093 patients (36%) experienced clinical inertia. After PSM, 1,760 patients remained; 880 in each group. In the clinical inertia group, 23% of patients achieved an A1c < 7.0% in the post-index period, compared with 35% in the treatment intensification group (P < 0.001). A greater likelihood of experiencing clinical inertia was associated with baseline treatment with 2 (OR = 1.51, 95% CI = 1.22-2.86; P < 0.001) or ≥ 3 (OR = 1.78, 95% CI = 1.30-2.42; P < 0.001) antihyperglycemic medications (vs. none), baseline age ≥ 65 years (OR = 2.11, 95% CI = 1.63-2.74; P < 0.001), and diagnosis of coronary heart disease (OR = 1.44, 95% CI = 1.10-1.88; P = 0.007). A baseline A1c ≥ 9.0% (vs. 8.0%-8.9%) was associated with a lower likelihood of experiencing clinical inertia (OR = 0.56, 95% CI = 0.48-0.66; P < 0.001).
Conclusions: More than a third of patients in a commercially insured population with T2DM and a baseline A1c ≥ 8% experienced clinical inertia. Clinical inertia resulted in worse A1c outcomes over the 12-month follow-up period. Results of this study suggest that treatment intensification should be monitored, with efforts made to educate health care providers on strategies aimed at improving glycemic control for high-risk patients.
Disclosures: This study was funded by a grant from Janssen Scientific Affairs, which was involved in study design, interpretation of results, and manuscript review. Wander reports consulting fees from Sanofi Aventis outside the submitted work. McAdam-Marx reports grants from Sanofi Aventis and AstraZeneca outside the submitted work. Pesa and Bailey were employees of Janssen Scientific Affairs during the conduct of the study. Bailey also reports stock ownership in Johnson and Johnson. This study was presented as a poster at the Academy of Managed Care Pharmacy Nexus 2017; October 16-19, 2017; Grapevine, TX.
Conflict of interest statement
This study was funded by a grant from Janssen Scientific Affairs, which was involved in study design, interpretation of results, and manuscript review. Wander reports consulting fees from Sanofi Aventis outside the submitted work. McAdam-Marx reports grants from Sanofi Aventis and AstraZeneca outside the submitted work. Pesa and Bailey were employees of Janssen Scientific Affairs during the conduct of the study. Bailey also reports stock ownership in Johnson and Johnson.
This study was presented as a poster at the Academy of Managed Care Pharmacy Nexus 2017; October 16-19, 2017; Grapevine, TX.
Figures
Similar articles
-
Influence of Treatment Intensification on A1c in Patients with Suboptimally Controlled Type 2 Diabetes After 2 Oral Antidiabetic Agents.J Manag Care Spec Pharm. 2019 Mar;25(3):314-322. doi: 10.18553/jmcp.2019.25.3.314. J Manag Care Spec Pharm. 2019. PMID: 30816811 Free PMC article.
-
Slow Titration and Delayed Intensification of Basal Insulin Among Patients with Type 2 Diabetes.J Manag Care Spec Pharm. 2018 Apr;24(4):390-400. doi: 10.18553/jmcp.2017.17218. Epub 2017 Nov 16. J Manag Care Spec Pharm. 2018. PMID: 29406841 Free PMC article.
-
Real-World Glycemic Control from GLP-1RA Therapy with and Without Concurrent Insulin in Patients with Type 2 Diabetes.J Manag Care Spec Pharm. 2017 Mar;23(3):267-275. doi: 10.18553/jmcp.2017.16334. Epub 2017 Feb 6. J Manag Care Spec Pharm. 2017. PMID: 28230449 Free PMC article.
-
Addressing Clinical Inertia in Type 2 Diabetes Mellitus: A Review.Adv Ther. 2018 Nov;35(11):1735-1745. doi: 10.1007/s12325-018-0819-5. Epub 2018 Oct 29. Adv Ther. 2018. PMID: 30374807 Free PMC article. Review.
-
Strategies to Overcome Therapeutic Inertia in Type 2 Diabetes Mellitus: A Scoping Review.Can J Diabetes. 2021 Apr;45(3):273-281.e13. doi: 10.1016/j.jcjd.2020.08.109. Epub 2020 Sep 7. Can J Diabetes. 2021. PMID: 33160883
Cited by
-
Temporal trends in the starting of insulin therapy in type 2 diabetes in Italy: data from the AMD Annals initiative.J Endocrinol Invest. 2024 Aug;47(8):2087-2096. doi: 10.1007/s40618-024-02306-5. Epub 2024 Mar 5. J Endocrinol Invest. 2024. PMID: 38441838 Free PMC article.
-
Clinical Inertia in the Management of Type 2 Diabetes Mellitus: A Systematic Review.Medicina (Kaunas). 2023 Jan 16;59(1):182. doi: 10.3390/medicina59010182. Medicina (Kaunas). 2023. PMID: 36676805 Free PMC article.
-
Delays in Insulin Initiation among Patients with Type 2 Diabetes Mellitus in Southeast China: A Retrospective, Real-World Study.Diabetes Metab Syndr Obes. 2020 Aug 25;13:3059-3068. doi: 10.2147/DMSO.S256381. eCollection 2020. Diabetes Metab Syndr Obes. 2020. PMID: 32922056 Free PMC article.
-
Predictors of Clinical Inertia and Type 2 Diabetes: Assessment of Primary Care Physicians and Their Patients.Int J Environ Res Public Health. 2022 Apr 7;19(8):4436. doi: 10.3390/ijerph19084436. Int J Environ Res Public Health. 2022. PMID: 35457303 Free PMC article.
-
Clinical inertia and treatment intensification among patients with type ii diabetes mellitus at Debre Tabor comprehensive specialized hospital, Ethiopia: an institutional-based cross-sectional study.Front Endocrinol (Lausanne). 2025 Feb 6;16:1450928. doi: 10.3389/fendo.2025.1450928. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 39980847 Free PMC article.
References
-
- American Diabetes Association. Statistics about diabetes. 2017. Available at: http://www.diabetes.org/diabetes-basics/statistics/. Accessed December 22, 2018.
-
- Khaw KT, Wareham N, Bingham S, Luben R, Welch A, Day N. Association of hemoglobin A1c with cardiovascular disease and mortality in adults: the European prospective investigation into cancer in Norfolk. Ann Intern Med. 2004;141(6):413-20. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34). Lancet. 1998;352(9131):854-65. - PubMed
-
- American Diabetes Association. Standards of medical care in diabetes 2018. Diabetes Care. 2018;41(Suppl 1):S1-S155. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
