

Bone mineral density and estimated hip strength in men with anorexia nervosa, atypical anorexia nervosa and avoidant/restrictive food intake disorder
- PMID: 30817009
- PMCID: PMC6615544
- DOI: 10.1111/cen.13960
Bone mineral density and estimated hip strength in men with anorexia nervosa, atypical anorexia nervosa and avoidant/restrictive food intake disorder
Abstract
Objective: Few bone mineral density (BMD) data are available in men with anorexia nervosa (AN), and none in those with atypical AN (ATYP) (AN psychological symptoms without low weight) or avoidant/restrictive food intake disorder (ARFID) (restrictive eating without AN psychological symptoms). We investigated the prevalence and determinants of low BMD and estimated hip strength in men with these disorders.
Design: Cross-sectional: two centres.
Patients: A total of 103 men, 18-63 years: AN (n = 26), ARFID (n = 11), ATYP (n = 18), healthy controls (HC) (n = 48).
Measurements: Body composition, BMD and estimated hip strength (section modulus and buckling ratio) by DXA (Hologic). Serum 25OH vitamin D was quantified, as was daily calcium intake in a subset of subjects.
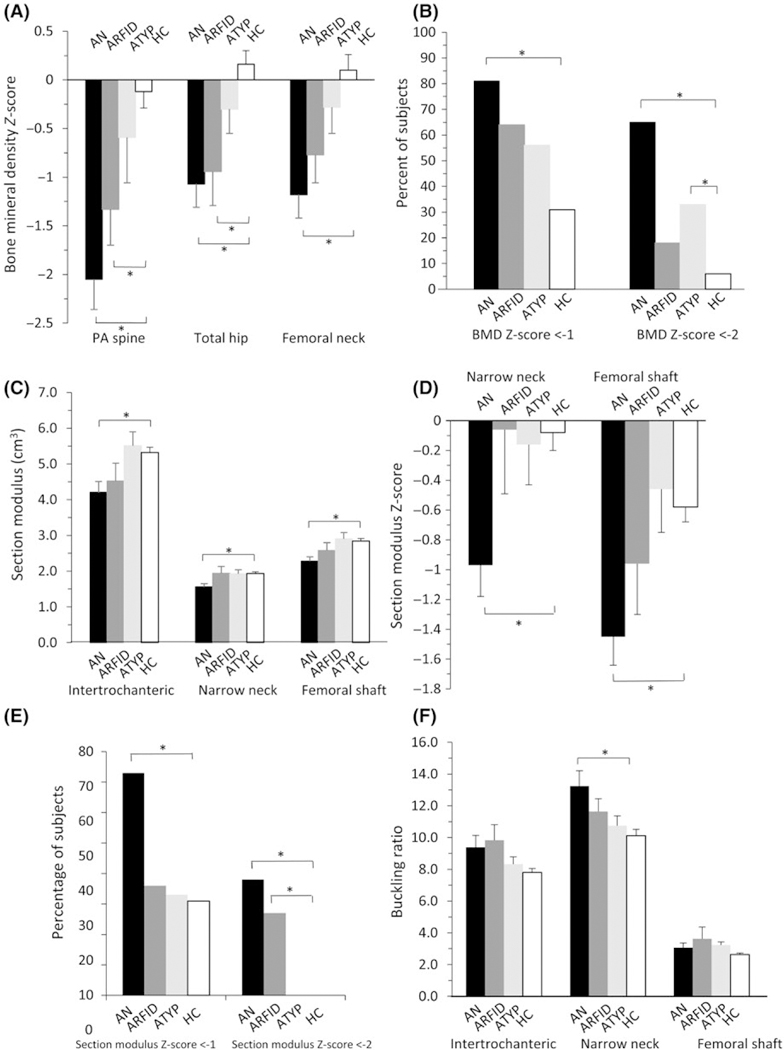
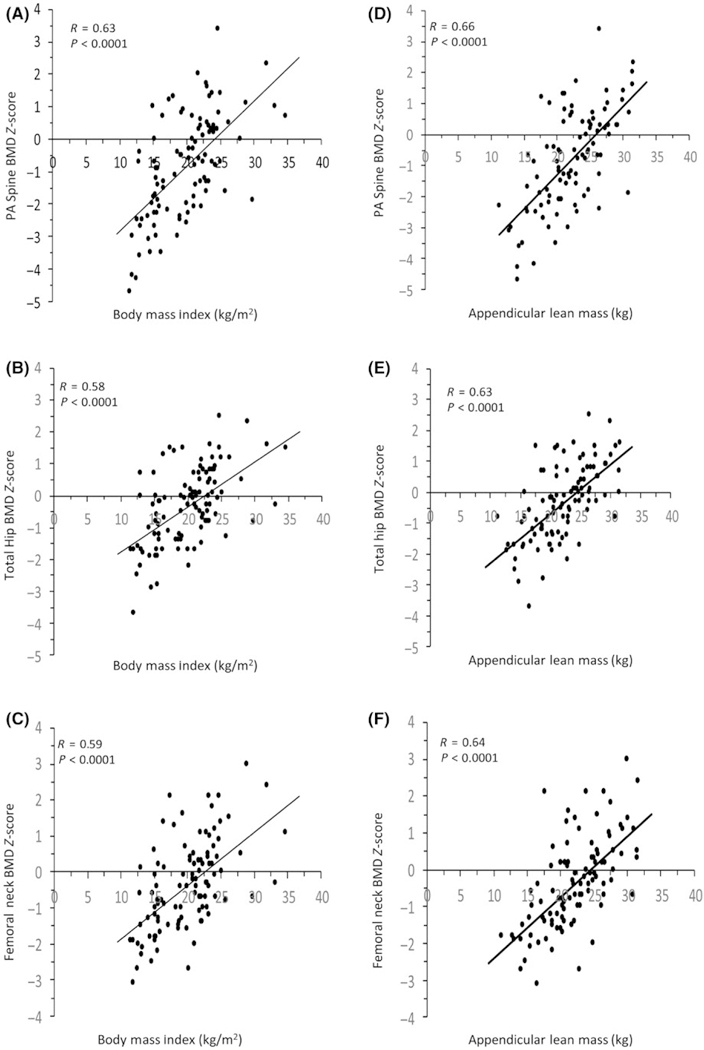
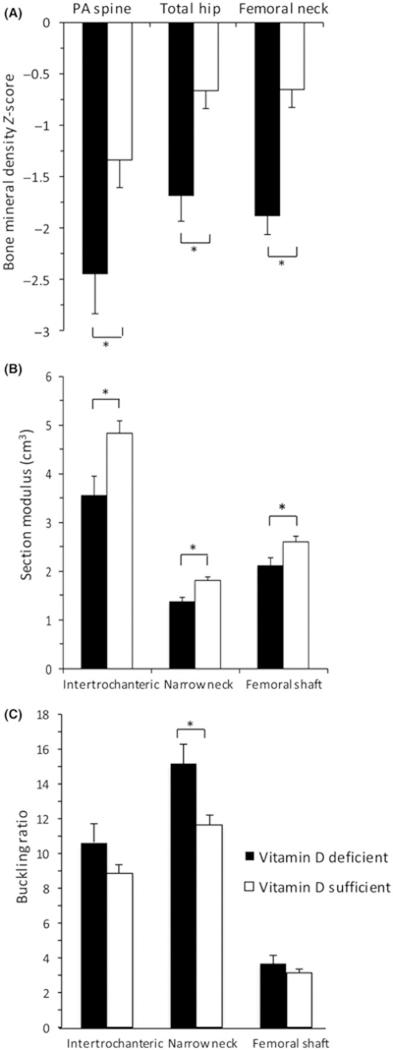
Results: Mean BMI was lowest in AN and ARFID, higher in ATYP and highest in HC (AN 14.7 ± 1.8, ARFID 15.3 ± 1.5, ATYP 20.6 ± 2.0, HC 23.7 ± 3.3 kg/m2 ) (P < 0.0005). Mean BMD Z-scores at spine and hip were lower in AN and ARFID, but not ATYP, than HC (postero-anterior (PA) spine AN -2.05 ± 1.58, ARFID -1.33 ± 1.21, ATYP -0.59 ± 1.77, HC -0.12 ± 1.17) (P < 0.05). 65% AN, 18% ARFID, 33% ATYP and 6% HC had BMD Z-scores <-2 at ≥1 site (AN and ATYP vs HC, P < 0.01). Mean section modulus Z-scores were lower in AN than HC (P < 0.01). Lower BMI, muscle mass and vitamin D levels (R = 0.33-0.64), as well as longer disease duration (R = -0.51 to -0.58), were associated with lower BMD (P < 0.05).
Conclusions: Men with AN, ARFID and ATYP are at risk for low BMD. Men with these eating disorders who are low weight, or who have low muscle mass, long illness duration and/or vitamin D deficiency, may be at particularly high risk.
Keywords: anorexia nervosa; bone density; feeding and eating disorders; vitamin D deficiency.
© 2019 John Wiley & Sons Ltd.
Conflict of interest statement
CONFLICT OF INTEREST
KTE reports future royalties for
Figures
Similar articles
-
Bone health in avoidant/restrictive food intake disorder: a narrative review.J Eat Disord. 2023 Mar 22;11(1):44. doi: 10.1186/s40337-023-00766-3. J Eat Disord. 2023. PMID: 36949522 Free PMC article. Review.
-
Bone mineral density in Anorexia Nervosa versus Avoidant Restrictive Food Intake Disorder.Bone. 2020 May;134:115307. doi: 10.1016/j.bone.2020.115307. Epub 2020 Mar 4. Bone. 2020. PMID: 32142910
-
Low bone mineral density is found in low weight female youth with avoidant/restrictive food intake disorder and associated with higher PYY levels.J Eat Disord. 2023 Jul 1;11(1):106. doi: 10.1186/s40337-023-00822-y. J Eat Disord. 2023. PMID: 37393263 Free PMC article.
-
Ghrelin and PYY in low-weight females with avoidant/restrictive food intake disorder compared to anorexia nervosa and healthy controls.Psychoneuroendocrinology. 2021 Jul;129:105243. doi: 10.1016/j.psyneuen.2021.105243. Epub 2021 Apr 28. Psychoneuroendocrinology. 2021. PMID: 34049199 Free PMC article.
-
Associations between bone mineral density, body composition and amenorrhoea in females with eating disorders: a systematic review and meta-analysis.J Eat Disord. 2022 Nov 18;10(1):173. doi: 10.1186/s40337-022-00694-8. J Eat Disord. 2022. PMID: 36401318 Free PMC article. Review.
Cited by
-
A Comprehensive Review of Complications and New Findings Associated with Anorexia Nervosa.J Clin Med. 2021 Jun 9;10(12):2555. doi: 10.3390/jcm10122555. J Clin Med. 2021. PMID: 34207744 Free PMC article. Review.
-
Dilemmas in the Management of Osteoporosis in Younger Adults.JBMR Plus. 2022 Jan 19;6(1):e10594. doi: 10.1002/jbm4.10594. eCollection 2022 Jan. JBMR Plus. 2022. PMID: 35079682 Free PMC article. Review.
-
Body composition in anorexia nervosa: Meta-analysis and meta-regression of cross-sectional and longitudinal studies.Int J Eat Disord. 2019 Nov;52(11):1205-1223. doi: 10.1002/eat.23158. Epub 2019 Sep 12. Int J Eat Disord. 2019. PMID: 31512774 Free PMC article. Review.
-
Bone health in avoidant/restrictive food intake disorder: a narrative review.J Eat Disord. 2023 Mar 22;11(1):44. doi: 10.1186/s40337-023-00766-3. J Eat Disord. 2023. PMID: 36949522 Free PMC article. Review.
-
Vitamin D and hypophosphatemia in patients with anorexia nervosa and avoidant/restrictive food intake disorder: a case control study.J Eat Disord. 2023 Nov 2;11(1):195. doi: 10.1186/s40337-023-00913-w. J Eat Disord. 2023. PMID: 37919813 Free PMC article.
References
-
- Melton LJ, Beck TJ, Amin S, et al. Contributions of bone density and structure to fracture risk assessment in men and women. Osteoporos Int. 2005;16(5):460–467. - PubMed
-
- American Psychiatric Association Publishing. Diagnostic and statistical manual of mental disorders (5th ed). In: Feeding and Eating Disorders. Washington, DC: American Psychiatric Publishing;2013:329–354
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
