

Once-weekly prophylaxis with glycoPEGylated recombinant factor VIII (N8-GP) in severe haemophilia A: Safety and efficacy results from pathfinder 2 (randomized phase III trial)
- PMID: 30817066
- PMCID: PMC6850405
- DOI: 10.1111/hae.13712
Once-weekly prophylaxis with glycoPEGylated recombinant factor VIII (N8-GP) in severe haemophilia A: Safety and efficacy results from pathfinder 2 (randomized phase III trial)
Abstract
Introduction: Turoctocog alfa pegol (N8-GP) is a site-specific, 40 kDa glycoPEGylated recombinant factor VIII (FVIII) product with an extended half-life. The comprehensive main phase of the pivotal pathfinder 2 trial showed N8-GP dosed every 4 days (Q4D) provided favourable safety and efficacy for preventing bleeds in 175 patients with haemophilia A.
Aim and methods: We investigated the safety and efficacy of N8-GP prophylaxis when administered weekly (Q7D) for 24 weeks to patients with low bleeding rates in the pathfinder 2 extension trial. Patients (≥12 years) with ≤2 bleeds during the preceding 6 months of the pathfinder 2 main phase were eligible for randomization to receive N8-GP 50 IU/kg Q4D or 75 IU/kg Q7D. Safety and efficacy endpoints were incidence of FVIII inhibitors and annualized bleeding rate (ABR), respectively.
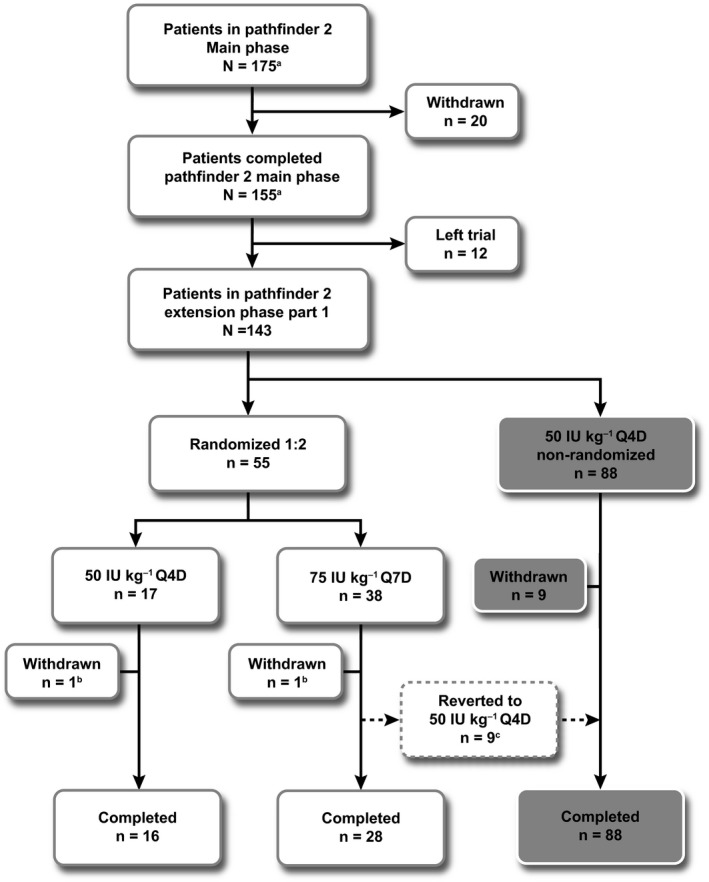
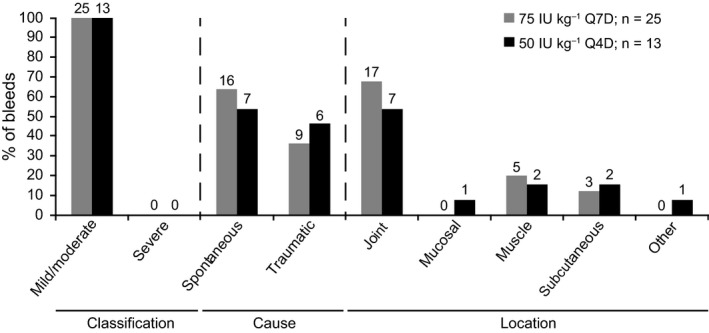
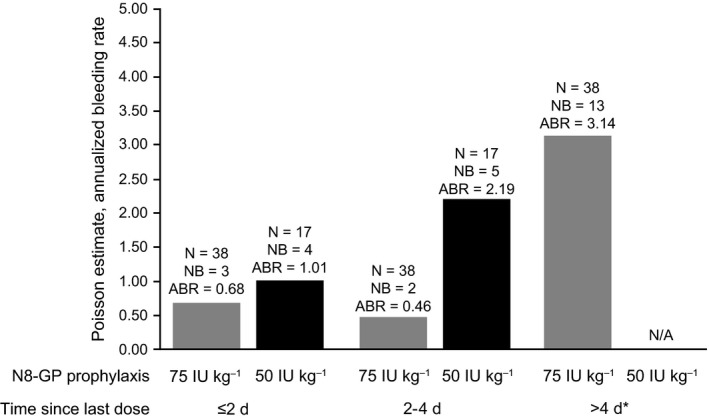
Results: Fifty-five of 143 (38.5%) patients on prophylaxis who continued into the extension phase were randomized to receive 50 IU/kg Q4D (n = 17) or 75 IU/kg Q7D (n = 38). Nine patients in the Q7D cohort reverted to 50 IU/kg Q4D. No inhibitors were detected. In both cohorts, >50% of patients experienced no bleeds. Median ABR for overall, joint, spontaneous, traumatic and muscle was 0.00 for both cohorts. Overall estimated success rate for treating bleeding episodes was 87.5%; 94.7% of bleeds were controlled with ≤2 injections.
Conclusions: Weekly N8-GP was well tolerated and efficacious and may benefit selected "low bleeder" patients with haemophilia A.
Keywords: FVIII; N8-GP; efficacy; haemophilia A; once-weekly prophylaxis; safety.
© 2019 The Authors. Haemophilia Published by John Wiley & Sons Ltd.
Conflict of interest statement
NC has received support to attend conferences from Bayer, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Shire and SOBI, and advisory boards from LFB, Shire and SOBI. She has served as a paid consultant for Bayer and was the Investigator who led research for CSL Behring. CA has received research support from Bayer, Octapharma, Pfizer and Shire, and has served as a paid consultant for Bayer, Biogen Idec, CSL Behring, Novo Nordisk, Pfizer, Shire and SOBI. ME has received research support from Pfizer and has served as a paid consultant for Bayer, CSL Behring, Genentech, Hemabiologics, Kedrion, Novo Nordisk, Octapharma, Pfizer and Shire. PAH received research support from Bayer, Octapharma, Pfizer and Shire, and has served as a paid consultant for Bayer, Biogen Idec, CSL Behring, Novo Nordisk, Pfizer, Shire and SOBI. SK received a grant from Bayer, Bioverativ, Daiichi Sankyo, Grifols and Novo Nordisk, and attended advisory boards for Bayer, Bioverativ and Novo Nordisk. RK received research support from Baxalta (Shire), Bayer, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Shire and SOBI, and has served as a paid consultant for Baxalta (Shire), Bayer, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Shire and SOBI. MM has nothing to disclose. CN received research support and/or was a Principal Investigator for Alnylam, Baxalta (Shire), Bayer, Biogen Idec/SOBI, CSL Behring, Novo Nordisk, Octapharma and Pfizer. He attended scientific advisory boards and received honoraria and/or travel support from Baxalta (Shire), Bayer, Biogen Idec/SOBI, CSL Behring, LFB, Novo Nordisk, Octapharma and Pfizer. AW participated in advisory boards for Baxalta (Shire), Novo Nordisk, Octapharma and Bayer. ES attended and received funds for advisory boards from Bayer, Grifols, Kedrion, Novo Nordisk, Octapharma, Pfizer, Roche, Shire and SOBI. She attended Speaker Bureaus for and received funds from Bayer, Bioverativ, CSL Behring, Grifols, Kedrion, Novo Nordisk, Octapharma, Pfizer, Roche, Shire and SOBI. MS has received grant support from Bayer, Bioverativ, Chugai, CSL Behring, Novo Nordisk, Pfizer, Roche and Shire; personal fees from Bayer, Bioverativ, Chugai, Novo Nordisk, Sysmex and Shire. AL and SMT are employees of Novo Nordisk A/S. SRL has received grant support and personal fees from Novo Nordisk A/S and has served as a paid consultant for Novo Nordisk A/S.
Figures
References
-
- Manco‐Johnson MJ, Abshire TC, Shapiro AD, et al. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. N Engl J Med. 2007;357:535‐544. - PubMed
-
- Zappa S, McDaniel M, Marandola J, Allen G. Treatment trends for haemophilia A and haemophilia B in the United States: results from the 2010 practice patterns survey. Haemophilia. 2012;18:e140‐e153. - PubMed
-
- Srivastava A, Brewer AK, Mauser‐Bunschoten EP, et al. Guidelines for the management of hemophilia. Haemophilia. 2013;19:e1‐47. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
