

Implications of the Fracture Risk Assessment Algorithm for the assessment and improvement of bone health in patients with prostate cancer: A comprehensive review
- PMID: 30817274
- PMCID: PMC6619849
- DOI: 10.5152/tud.2019.11736
Implications of the Fracture Risk Assessment Algorithm for the assessment and improvement of bone health in patients with prostate cancer: A comprehensive review
Abstract
Objective: Maintaining the optimum bone health is one of the important concerns in patients with prostate cancer, but it usually remains neglected. Failure to screen these patients is detrimental to both the length and the quality of life. The estimation of bone mineral density (BMD) and more recently the World Health Organization's fracture risk assessment (FRAX) algorithm in appropriate patients is recommended by several specialty organizations/associations at the time of instituting androgen deprivation therapy (ADT) for metastatic and high-risk individuals. It provides a 10-year risk evaluation of hip and major osteoporotic fractures (MOF). Using this web-based new investigating tool, candidates at high risk of fractures can be predicted more accurately according to clinical risk factors (CRF) alone or in combination with the femoral neck BMD. The FRAX application for senile osteoporosis has been studied and reviewed extensively, but no systematic review has ever been conducted for assessing the implication of FRAX in prostate cancer. This review article will give insight about the validity, role, and utility of this investigating tool in clinical practice for fracture risk assessment in these individuals.
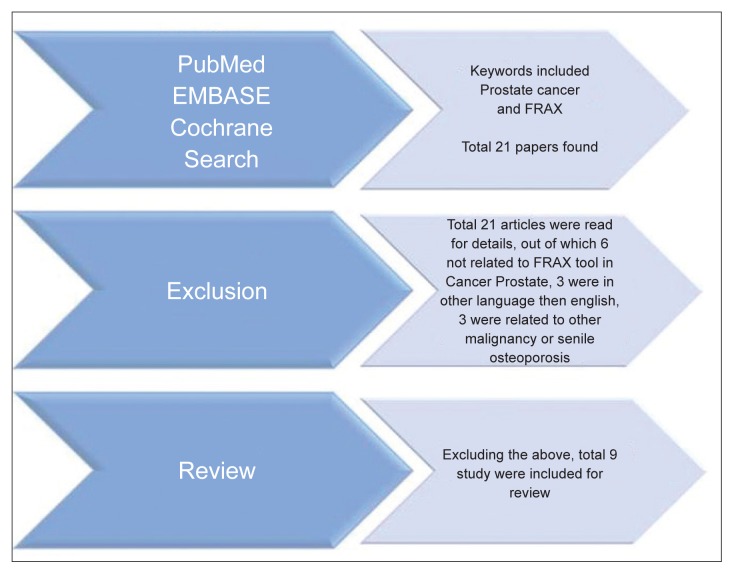
Material and methods: This systematic review was carried out as per the Preferred Reporting Items for Systematic Reviews and Meta-analyses guidelines and Cochrane review principles. We searched the PubMed, Cochrane database of systematic reviews, and the EMBASE electronic database until December 2018 using the medical subject heading terms prostate cancer and FRAX.
Results: A total of nine studies meet the inclusion criteria and were included in the review. These studies enrolled a total of 3704 patients (sample size range, 78-1220) of localized, metastatic, castration resistant prostate cancer with or without ADT and/or on photon or radiotherapy. The factors that influenced FRAX included age, ethnicity, baseline BMD, duration of ADT, presence of CRF, and measurement methods (CRF, with/without BMD, computed tomography based). An advanced age and duration of ADT were the most robust risk factors. A 10-year MOF and hip fracture risk estimation was higher when the femoral neck BMD was not incorporated in the FRAX measurement. Despite several well-known strengths of using FRAX in the fracture risk assessment of suitable candidates with prostate cancer, several risk factors such as the mode/duration of ADT, mode of radiotherapy, Vitamin D levels, bone remodeling markers, and recent/recurrent fractures need to be incorporated in the FRAX calculator for improving the predictive ability. In contrast to senile osteoporosis with a longer life expectancy, the fracture risk in patients with prostate cancer need to be measured more frequently and for a shorter time. Therefore, models like Garvan calculator with both 5- and 10-year risk estimates have to be developed for these patients. Additionally, its utilization is of limited value in the presence of recurrent fractures or falls.
Conclusion: The FRAX algorithm is beneficial in identifying patients who require early intervention or bone-directed therapy as an early step to decrease skeletal-related events and other morbidity. Several risk factors need to be added for improving the FRAX predictive value. This model is still underutilized in the clinical practice and increasing the awareness among treating physicians will help in optimizing the bone health and the quality of life of this important population subgroup.
Conflict of interest statement
Figures
Similar articles
-
A prospective longitudinal study to evaluate bone health, implication of FRAX tool and impact on quality of life (FACT-P) in advanced prostate cancer patients.Am J Clin Exp Urol. 2021 Jun 15;9(3):211-220. eCollection 2021. Am J Clin Exp Urol. 2021. PMID: 34327260 Free PMC article.
-
Improving bone health in prostate cancer patients starting androgen deprivation therapy: does Fracture Risk Assessment Tool (FRAX®) enhance stratification and targeted management?Arch Osteoporos. 2022 Nov 15;17(1):143. doi: 10.1007/s11657-022-01185-8. Arch Osteoporos. 2022. PMID: 36376762
-
Utilization of DXA Bone Mineral Densitometry in Ontario: An Evidence-Based Analysis.Ont Health Technol Assess Ser. 2006;6(20):1-180. Epub 2006 Nov 1. Ont Health Technol Assess Ser. 2006. PMID: 23074491 Free PMC article.
-
Performance of predictive tools to identify individuals at risk of non-traumatic fracture: a systematic review, meta-analysis, and meta-regression.Osteoporos Int. 2019 Apr;30(4):721-740. doi: 10.1007/s00198-019-04919-6. Epub 2019 Mar 14. Osteoporos Int. 2019. PMID: 30877348
-
Use of Fracture Risk Assessment Tool in clinical practice and Fracture Risk Assessment Tool future directions.Womens Health (Lond). 2024 Jan-Dec;20:17455057241231387. doi: 10.1177/17455057241231387. Womens Health (Lond). 2024. PMID: 38529935 Free PMC article. Review.
Cited by
-
Compilation and Analysis of Web-Based Orthopedic Personalized Predictive Tools: A Scoping Review.J Pers Med. 2020 Nov 12;10(4):223. doi: 10.3390/jpm10040223. J Pers Med. 2020. PMID: 33198106 Free PMC article.
-
Efficacy and safety of darolutamide in Japanese patients with nonmetastatic castration-resistant prostate cancer: a sub-group analysis of the phase III ARAMIS trial.Int J Clin Oncol. 2021 Mar;26(3):578-590. doi: 10.1007/s10147-020-01824-5. Epub 2020 Nov 23. Int J Clin Oncol. 2021. PMID: 33226524 Free PMC article. Clinical Trial.
References
-
- Smith MR, Brown GA, Saad F. New opportunities in the management of prostate cancer related bone complications. Urologic Oncology: Seminars and Original Investigations. 2009;27:S1–20.
Publication types
LinkOut - more resources
Full Text Sources