

The impact of a muscle pump activator on incisional wound healing compared to standard stockings and compression devices in kidney and kidney-pancreas transplant recipients: A randomized controlled trial
- PMID: 30817287
- PMCID: PMC6877366
- DOI: 10.5489/cuaj.5822
The impact of a muscle pump activator on incisional wound healing compared to standard stockings and compression devices in kidney and kidney-pancreas transplant recipients: A randomized controlled trial
Abstract
Introduction: We aimed to evaluate the impact of thrombo-embolic-deterrent + intermittent pneumatic compression (TED + IPC) vs. muscle pump activator (MPA) on incisional wound healing in kidney and simultaneous pancreas- kidney (SPK) transplant recipients.
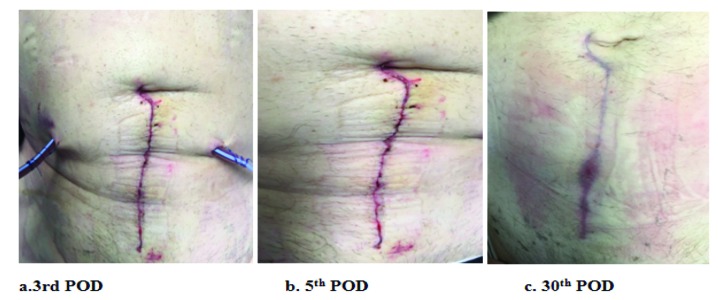
Methods: We conducted a single-centre, randomized controlled trial in which 104 patients (kidney n=94; SPK n=10) were randomly assigned to wear TED + IPC (n= 52) or MPA (n=52) for the first six days following surgery. Patient demographics, postoperative outcomes, and incisional wound images were taken using a HIPAA-compliant application on postoperative days (POD) 3, 5, and 30, and assessed using the validated Southampton Wound Care Score.
Results: There were no demographic differences between the groups. The MPA group had a significant improvement in wound healing on POD 3 (p=0.04) that persisted until POD 5 (p=0.0003). At POD 30, both groups were similar in wound healing outcomes (p=0.51). Bayesian inferential analysis revealed that the use of TED + IPC following transplantation had inferior outcomes compared to the use of MPA with sequential moderate evidence. The rate of complex wound infections was significantly greater in the TED + IPC group compared to the MPA group (29% vs. 12%, respectively; p=0.03). Patients were more satisfied with the use of a MPA device than TED + IPC. No major complications were encountered in either group.
Conclusions: The use of a MPA device in the immediate postoperative period leads to a significant improvement in immediate and early wound healing, and decreased number of complex wound infections following kidney and SPK transplantation compared to standard TED + IPC therapy. Patients were more satisfied with the use of a MPA device than TED + IPC.
Conflict of interest statement
Figures








Similar articles
-
Daily use of a muscle pump activator device reduces duration of hospitalization and improves early graft outcomes post-kidney transplantation: A randomized controlled trial.Can Urol Assoc J. 2021 Feb;15(2):26-32. doi: 10.5489/cuaj.6487. Can Urol Assoc J. 2021. PMID: 32745003 Free PMC article.
-
Use of a Muscle Pump Activator Leads to Improved Lower Limb Edema, Lower Limb Blood Flow, and Urine Output Compared With Standard TED Stockings and Compression Devices Following Kidney Transplant: A Randomized Controlled Trial.Transplant Proc. 2019 Jul-Aug;51(6):1838-1844. doi: 10.1016/j.transproceed.2019.04.032. Epub 2019 Jun 27. Transplant Proc. 2019. PMID: 31256870 Clinical Trial.
-
Pancreas after kidney transplants.Am J Surg. 2001 Aug;182(2):155-61. doi: 10.1016/s0002-9610(01)00676-6. Am J Surg. 2001. PMID: 11574088
-
Optimal surgical management in kidney and pancreas transplantation to minimise wound complications: A systematic review and meta-analysis.Ann Med Surg (Lond). 2018 Aug 18;33:24-31. doi: 10.1016/j.amsu.2018.08.006. eCollection 2018 Sep. Ann Med Surg (Lond). 2018. PMID: 30167299 Free PMC article. Review.
-
Using a programmable pneumatic device with truncal therapy to facilitate wound healing: a case series.Ostomy Wound Manage. 2009 Mar;55(3):34-6, 38-40. Ostomy Wound Manage. 2009. PMID: 19359708 Review.
Cited by
-
Daily use of a muscle pump activator device reduces duration of hospitalization and improves early graft outcomes post-kidney transplantation: A randomized controlled trial.Can Urol Assoc J. 2021 Feb;15(2):26-32. doi: 10.5489/cuaj.6487. Can Urol Assoc J. 2021. PMID: 32745003 Free PMC article.
-
The muscle pump activator device: From evidence to lived experiences.Int Wound J. 2024 Aug;21(8):e14949. doi: 10.1111/iwj.14949. Int Wound J. 2024. PMID: 39072891 Free PMC article. Review.
References
-
- Khoury JA, Brennan DC. Infectious complications in kidney transplant recipients: Review of the literature. Saudi J Kidney Dis Transpl. 2005;16:453–97. - PubMed
LinkOut - more resources
Full Text Sources
