

Symptom, diagnosis and mortality among respiratory emergency medical service patients
- PMID: 30817792
- PMCID: PMC6395033
- DOI: 10.1371/journal.pone.0213145
Symptom, diagnosis and mortality among respiratory emergency medical service patients
Abstract
Objective: Breathing difficulties and respiratory diseases have been under-reported in Emergency Medical Services research, despite these conditions being prevalent with substantial mortality. Our aim was two-fold; 1) to investigate the diagnostic pattern and mortality among EMS patients to whom an ambulance was dispatched due to difficulty breathing, and 2) to investigate the initial symptoms and mortality for EMS patients diagnosed with respiratory diseases in hospital.
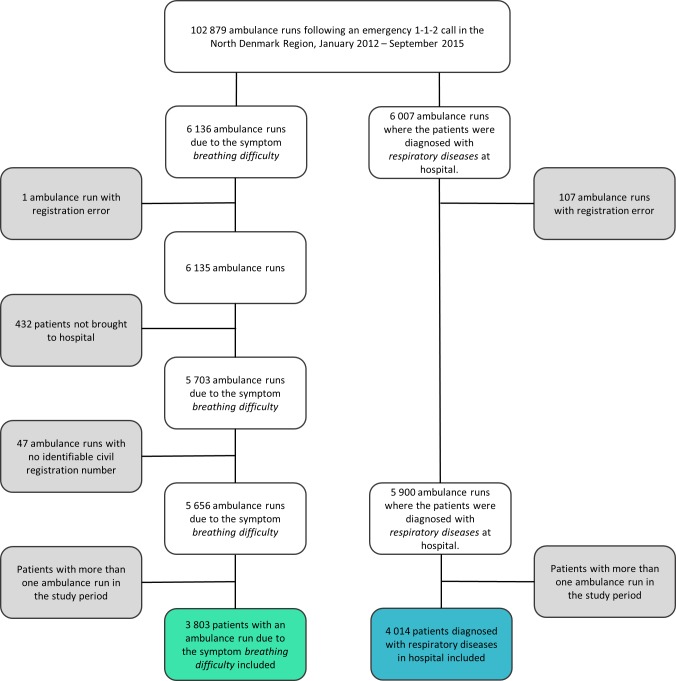
Methods: Population-based historic cohort study in the North Denmark Region 2012-2015. We included two patient groups; 1) patients calling the emergency number with breathing difficulty as main symptom, and 2) patients diagnosed with respiratory diseases in hospital following an emergency call. Main outcome was estimated 1- and 30-day mortality rates.
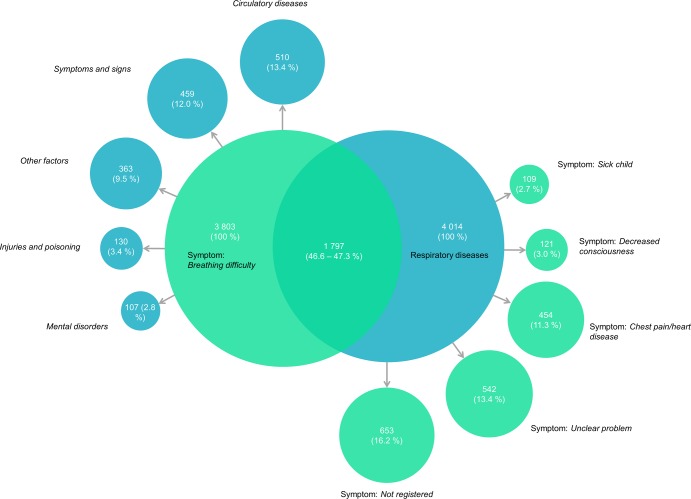
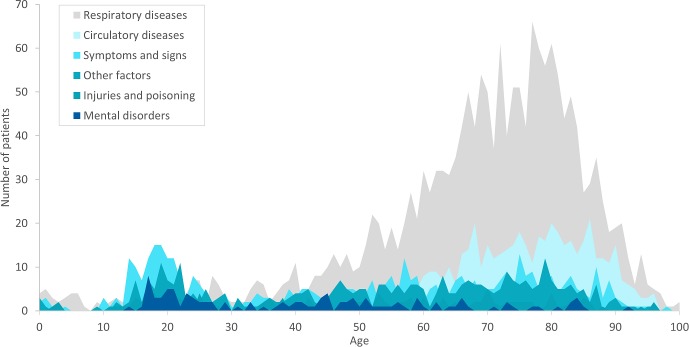
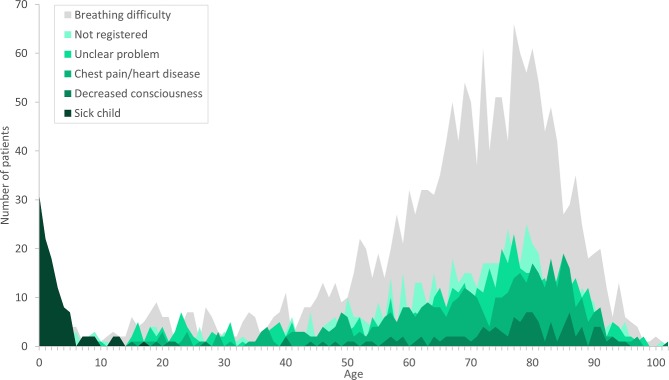
Results: There were 3803 patients with the symptom breathing difficulty, nearly half were diagnosed with respiratory diseases 47.3%, followed by circulatory diseases 13.4%, and symptoms and signs 12.0%. The 1-day mortality rate was highest for circulatory diseases, then respiratory diseases and other factors. Over-all 30-day mortality was 13.2%, and the highest rate was for circulatory diseases (17.7%) then respiratory diseases and other factors. A total of 4014 patients were diagnosed with respiratory diseases, 44.8% had the symptom breathing difficulty, 13.4% unclear problems and 11.3%. chest pain/heart disease. 1-day mortality rates were highest for decreased consciousness, then breathing difficulties and unclear problem. Over-all 30-day mortality rates were 12.5%, the highest with symptoms of decreased consciousness (19.1%), then unclear problem and breathing difficulty. There was an overlap of 1797 patients between the two groups.
Conclusions: The over-all mortality rates alongside the distribution of symptoms and diagnoses, suggest the breathing difficulty patient group is complex and has severe health problems. These findings may be able to raise awareness towards the patient group, and thereby increase focus on diagnostics and treatment to improve the patient outcome.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Krafft T, García Castrillo-Riesgo L, Edwards S, Fischer M, Overton J, Robertson-Steel I, et al. European Emergency Data Project (EED Project): EMS data-based health surveillance system. Eur J Public Health. 2003;13(3 Suppl):85–90. - PubMed
-
- Parshall MB, Schwartzstein RM, Adams L, Banzett RB, Manning HL, Bourbeau J, et al. An official American Thoracic Society statement: update on the mechanisms, assessment, and management of dyspnea. Am J Respir Crit Care Med. 2012. February 15;185(4):435–52. 10.1164/rccm.201111-2042ST - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
