

Real-time adaptive planning method for radiotherapy treatment delivery for prostate cancer patients, based on a library of plans accounting for possible anatomy configuration changes
- PMID: 30818345
- PMCID: PMC6394960
- DOI: 10.1371/journal.pone.0213002
Real-time adaptive planning method for radiotherapy treatment delivery for prostate cancer patients, based on a library of plans accounting for possible anatomy configuration changes
Abstract
Background and purpose: In prostate cancer treatment with external beam radiation therapy (EBRT), prostate motion and internal changes in tissue distribution can lead to a decrease in plan quality. In most currently used planning methods, the uncertainties due to prostate motion are compensated by irradiating a larger treatment volume. However, this could cause underdosage of the treatment volume and overdosage of the organs at risk (OARs). To reduce this problem, in this proof of principle study we developed and evaluated a novel adaptive planning method. The strategy proposed corrects the dose delivered by each beam according to the actual position of the target in order to produce a final dose distribution dosimetrically as similar as possible to the prescribed one.
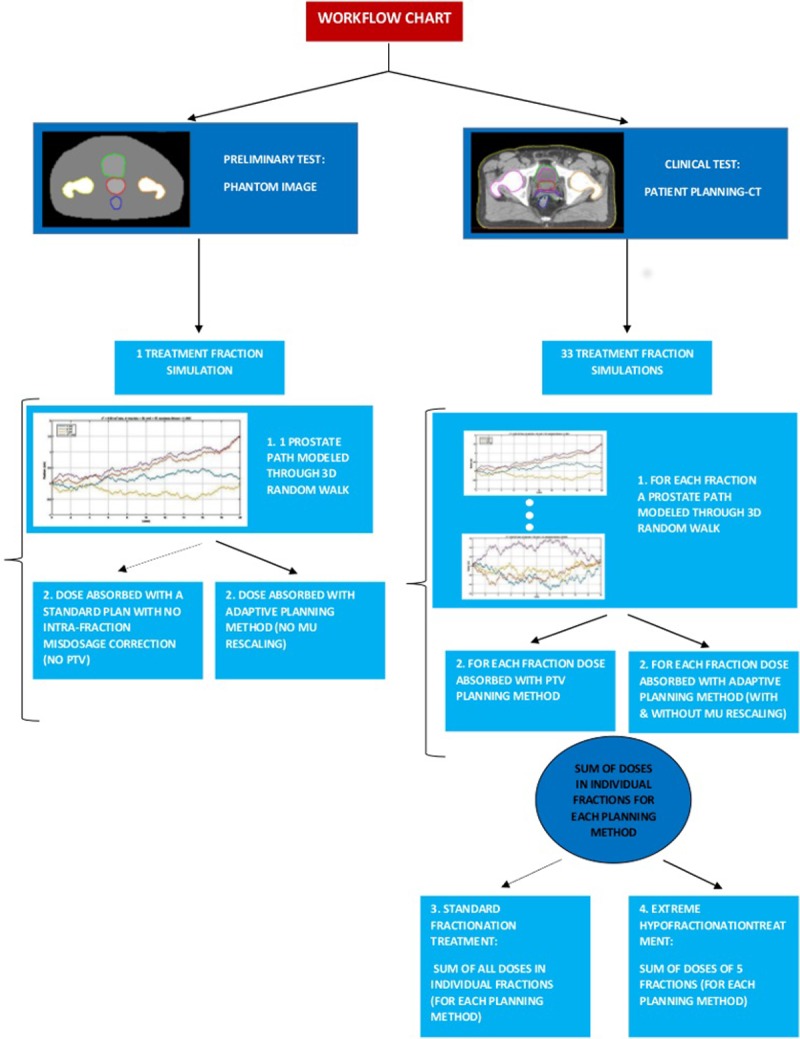
Material and methods: Our adaptive planning method was tested on a phantom case and on a clinical case. For the first, a pilot study was performed on an in-silico pelvic phantom. A "library" of intensity modulated RT (IMRT) plans corresponding to possible positions of the prostate during a treatment fraction was generated at planning stage. Then a 3D random walk model was used to simulate possible displacements of the prostate during the treatment fraction. At treatment stage, at the end of each beam, based on the current position of the target, the beam from the library of plans, which could reproduce the best approximation of the prescribed dose distribution, was selected and delivered. In the clinical case, the same approach was used on two prostate cancer patients: for the first a tissue deformation was simulated in-silico and for the second a cone beam CT (CBCT) taken during the treatment was used to simulate an intra-fraction change. Then, dosimetric comparisons with the standard treatment plan and, for the second patient, also with an isocenter shift correction, were performed.
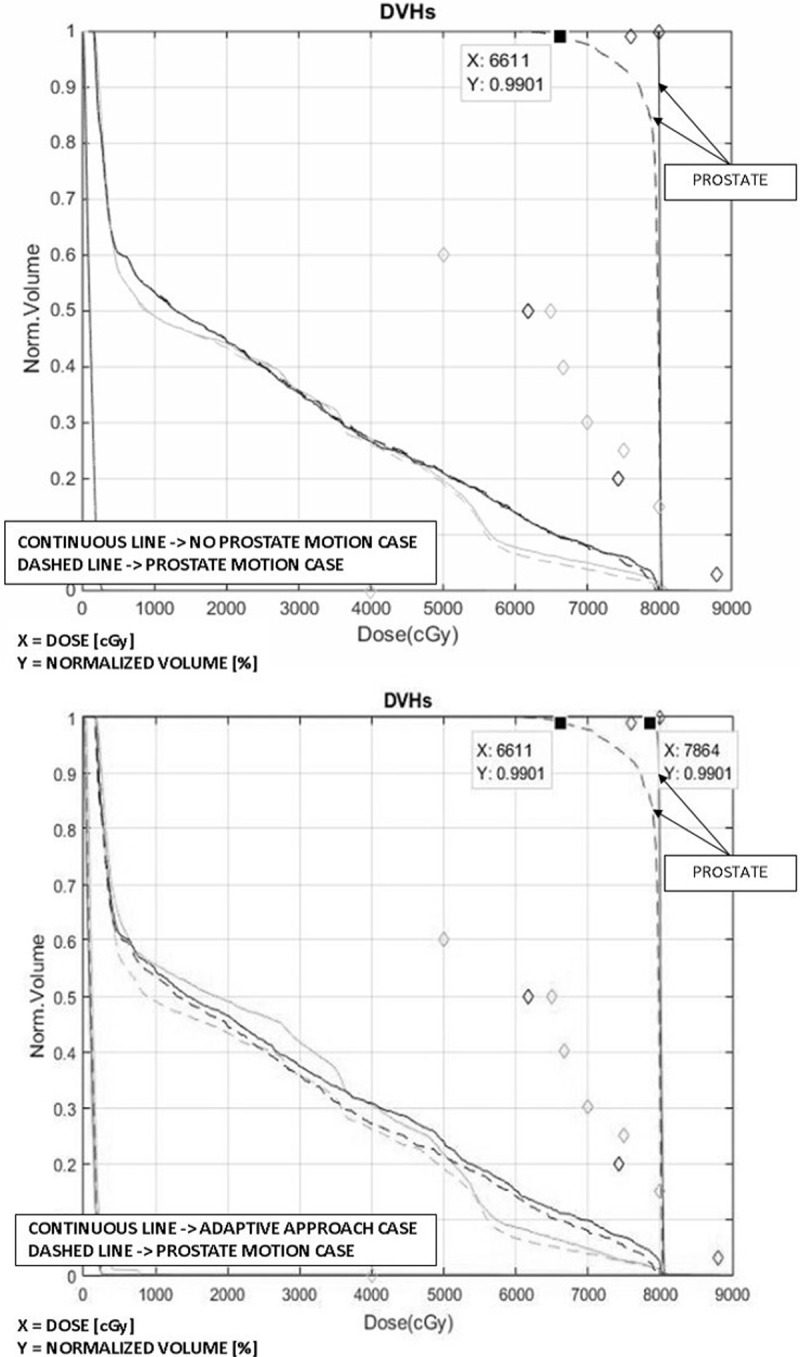
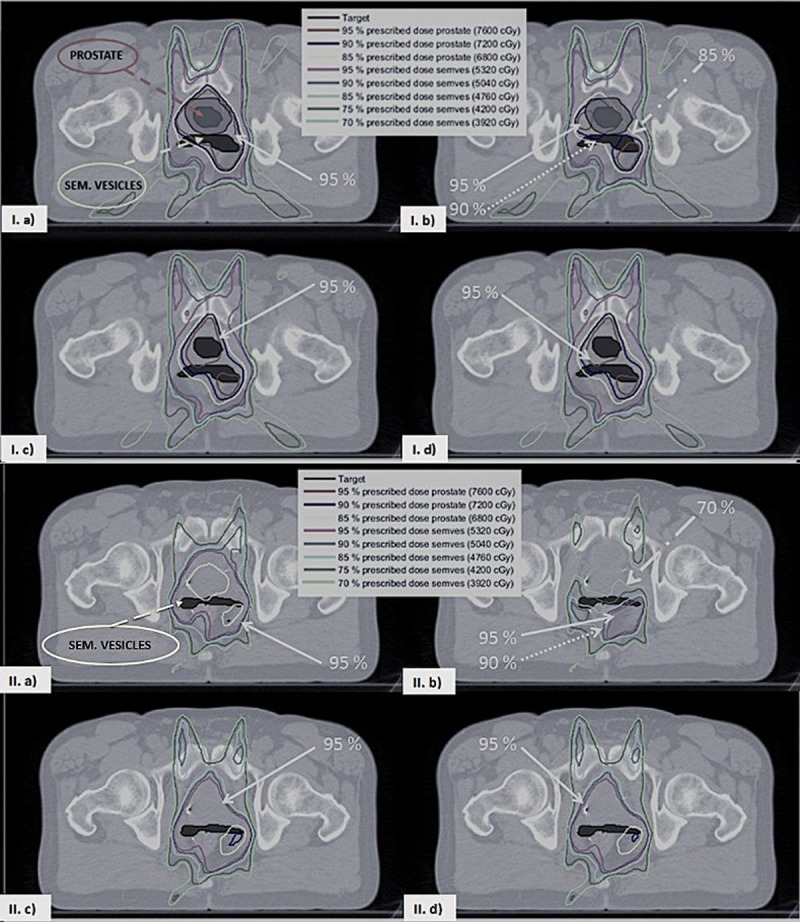
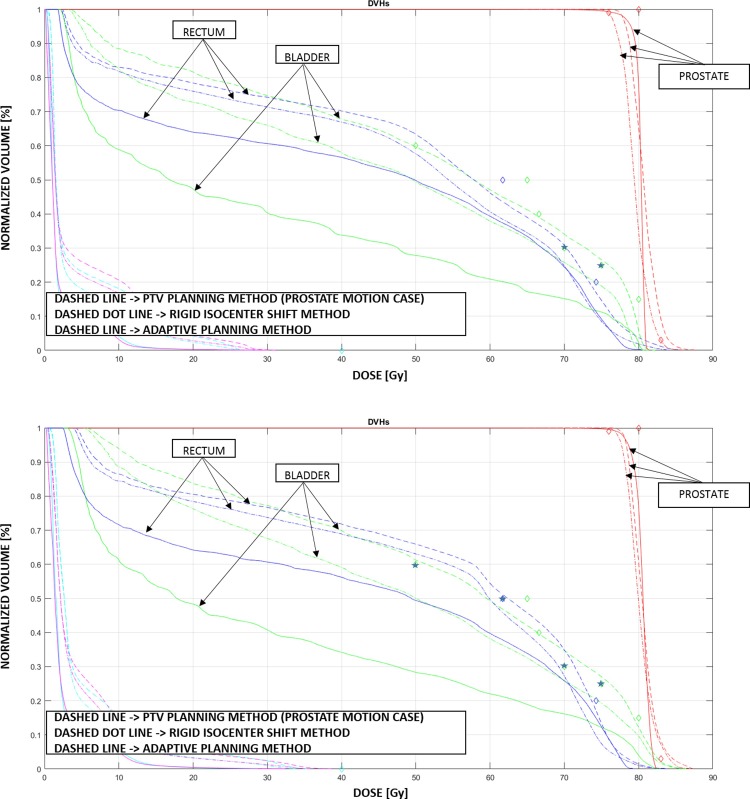
Results: For the phantom case, the plan generated using the adaptive planning method was able to meet all the dosimetric requirements and to correct for a misdosage of 13% of the dose prescription on the prostate. For the first clinical case, the standard planning method caused underdosage of the seminal vesicles, respectively by 5% and 4% of the prescribed dose, when the position changes for the target were correctly taken into account. The proposed adaptive planning method corrected any possible missed target coverage, reducing at the same time the dose on the OARs. For the second clinical case, both with the standard planning strategy and with the isocenter shift correction target coverage was significantly worsened (in particular uniformity) and some organs exceeded some toxicity objectives. While with our approach, the most uniform coverage for the target was produced and systematically the lowest toxicity values for the organs at risk were achieved.
Conclusions: In our proof of principle study, the adaptive planning method performed better than the standard planning and the isocenter shift methods for prostate EBRT. It improved the coverage of the treatment volumes and lowered the dose to the OARs. This planning method is particularly promising for hypofractionated IMRT treatments in which a higher precision and control on dose deposition are needed. Further studies will be performed to test more extensively the proposed adaptive planning method and to evaluate it at a full clinical level.
Conflict of interest statement
We have the following interests. All the authors were employed by Philips Research, when the work has been implemented. Presently, only Peter Prinsen and Alfonso A. Isola are employed by Philips Research. This work is related to an invention previously patented by two of the co-authors (“Radiation therapy system using plural treatment plans”, patent #WO 2017005758 A1, inventors DF and AAI). There are no further patents, products in development or marketed products to declare. The commercial affiliation does not alter our adherence to PLOS ONE policies on sharing data and materials. This work is related to an invention previously patented by two of the co-authors (patent #WO 2017005758 A1, inventors DF and AAI). This does not alter our adherence to PLOS ONE policies on sharing data and materials.
Figures
Similar articles
-
Dosimetric evaluation of three adaptive strategies for prostate cancer treatment including pelvic lymph nodes irradiation.Med Phys. 2015 Dec;42(12):7011-21. doi: 10.1118/1.4935529. Med Phys. 2015. PMID: 26632056
-
Evaluation of online/offline image guidance/adaptation approaches for prostate cancer radiation therapy.Int J Radiat Oncol Biol Phys. 2015 Apr 1;91(5):1026-33. doi: 10.1016/j.ijrobp.2014.12.043. Int J Radiat Oncol Biol Phys. 2015. PMID: 25832693
-
Towards automated on-line adaptation of 2-Step IMRT plans: QUASIMODO phantom and prostate cancer cases.Radiat Oncol. 2013 Nov 8;8:263. doi: 10.1186/1748-717X-8-263. Radiat Oncol. 2013. PMID: 24207129 Free PMC article.
-
A review of dose calculation approaches with cone beam CT in photon and proton therapy.Phys Med. 2020 Aug;76:243-276. doi: 10.1016/j.ejmp.2020.06.017. Epub 2020 Jul 28. Phys Med. 2020. PMID: 32736286 Review.
-
Image-guided Adaptive Radiotherapy for Bladder Cancer.Clin Oncol (R Coll Radiol). 2021 Jun;33(6):350-368. doi: 10.1016/j.clon.2021.03.023. Clin Oncol (R Coll Radiol). 2021. PMID: 33972024 Review.
Cited by
-
Comparison between Conventional IMRT Planning and a Novel Real-Time Adaptive Planning Strategy in Hypofractionated Regimes for Prostate Cancer: A Proof-of-Concept Planning Study.Healthcare (Basel). 2019 Dec 2;7(4):153. doi: 10.3390/healthcare7040153. Healthcare (Basel). 2019. PMID: 31810236 Free PMC article.
-
Artificial intelligence (AI) and interventional radiotherapy (brachytherapy): state of art and future perspectives.J Contemp Brachytherapy. 2020 Oct;12(5):497-500. doi: 10.5114/jcb.2020.100384. Epub 2020 Oct 30. J Contemp Brachytherapy. 2020. PMID: 33299440 Free PMC article. Review.
-
Personalized Treatment Planning Automation in Prostate Cancer Radiation Oncology: A Comprehensive Dosimetric Study.Front Oncol. 2021 Jun 1;11:636529. doi: 10.3389/fonc.2021.636529. eCollection 2021. Front Oncol. 2021. PMID: 34141608 Free PMC article.
-
Adipocytes protect fibroblasts from radiation-induced damage by adiponectin secretion.Sci Rep. 2020 Jul 28;10(1):12616. doi: 10.1038/s41598-020-69352-w. Sci Rep. 2020. PMID: 32724116 Free PMC article.
-
Technical feasibility of online adaptive stereotactic treatments in the abdomen on a robotic radiosurgery system.Phys Imaging Radiat Oncol. 2022 Jul 28;23:103-108. doi: 10.1016/j.phro.2022.07.005. eCollection 2022 Jul. Phys Imaging Radiat Oncol. 2022. PMID: 35928600 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
