

Evaluation of Xpert MTB-RIF guided diagnosis and treatment of rifampicin-resistant tuberculosis in Indonesia: A retrospective cohort study
- PMID: 30818352
- PMCID: PMC6394995
- DOI: 10.1371/journal.pone.0213017
Evaluation of Xpert MTB-RIF guided diagnosis and treatment of rifampicin-resistant tuberculosis in Indonesia: A retrospective cohort study
Abstract
Background: Rifampicin-resistant tuberculosis (RR-TB) is largely underdetected in Indonesia. Xpert MTB/RIF (Xpert) has recently been introduced, prioritizing patients at risk of RR-TB, followed by phenotypic drug-susceptibility (DST) if rifampicin resistance is detected.
Objective: This study investigated Xpert-based management of presumptive RR-TB cases under routine practice in West Java, Indonesia.
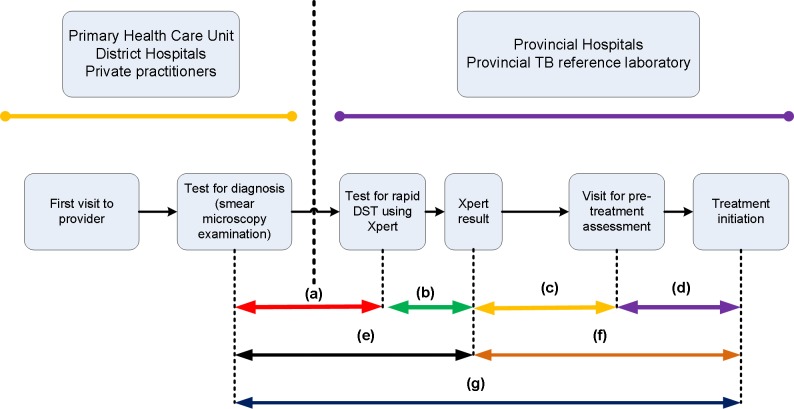
Methods: We examined all records of patients tested with Xpert in the referral hospital for West Java in 2015-2016. We measured loss across a limited cascade of care, time to Xpert diagnosis and the commencement of initial second-line treatment, and identified factors associated with diagnostic and treatment delay. Additionally, we analyzed the appropriateness of treatment according to DST results.
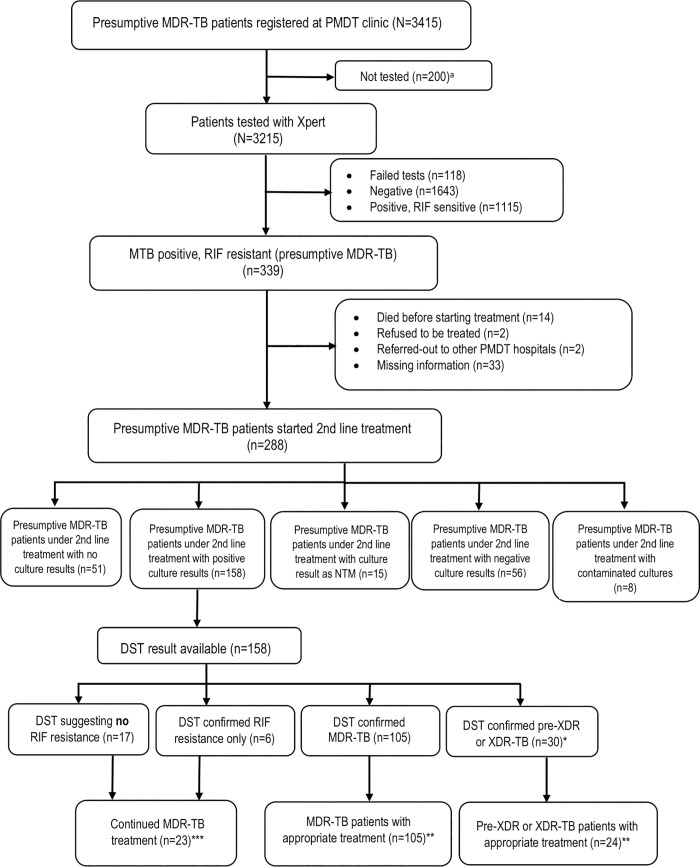
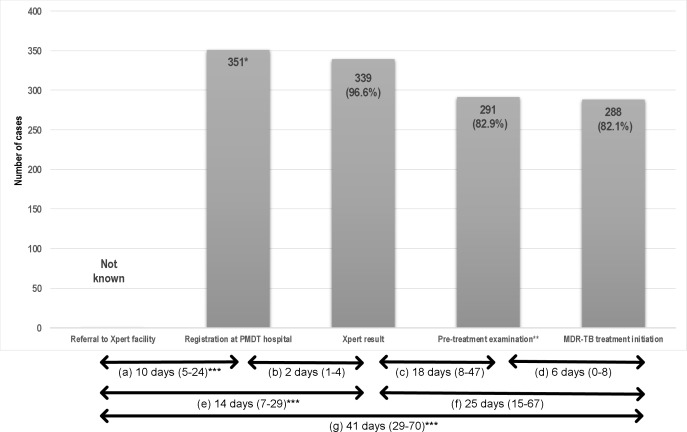
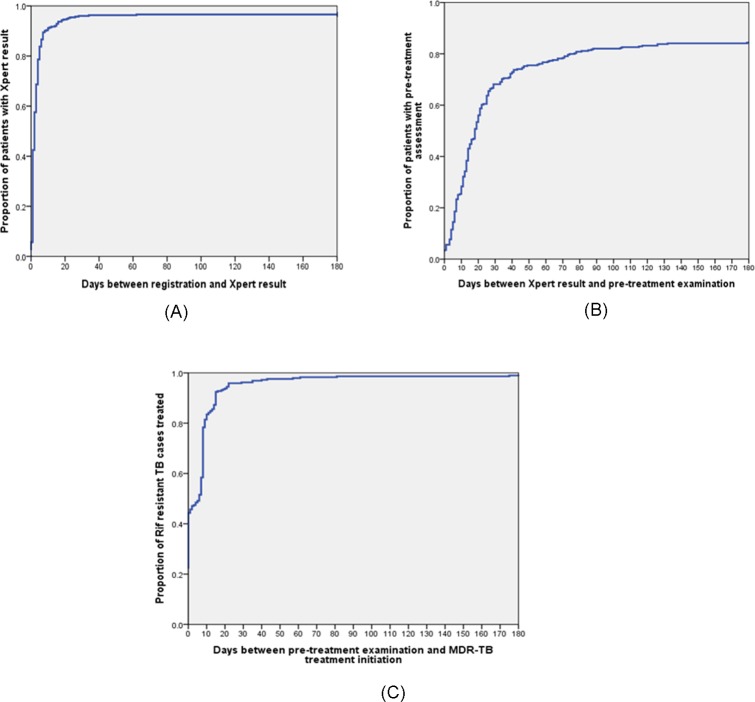
Results: Of 3415 patients with presumptive RR-TB, 3215 (94%) were tested by Xpert, of whom 339 (10.5%) were diagnosed as RR-TB. 288 (85%) of 339 RR-TB patients started initial second-line TB treatment, with 48 (14%) patients being lost between diagnosis and pre-treatment assessment. Second-line treatment was commenced at a median of 41 days (IQR 29-70) after RR-TB diagnosis. Delays in both diagnosis and treatment initiation were observed in 104 (52%) of 201 RR-TB patients with identifiable referral date. Rural residence was associated with delay to diagnosis (adjusted OR 2.7; 95%CI 1.5-5.2) and treatment initiation (adjusted OR 2.0; 1.2-3.4). Of 162 patients with available DST result, 107 (66%) had multidrug-resistant tuberculosis (MDR-TB) and 32 (20%) had either pre-extensively drug resistant (pre-XDR) or extensively drug resistant tuberculosis (XDR-TB). We estimated that with the current algorithm 41% of pre-XDR or XDR-TB patients are diagnosed, and 33% of them started on an appropriate treatment regimen.
Conclusions: Many patients with Xpert-diagnosed RR-TB either do not start MDR-TB treatment or encountered diagnostic and treatment delays under programmatic conditions in Indonesia, and most pre-XDR and XDR-TB cases remain undiagnosed. Further expansion and ongoing quality improvement of RR-TB services are urgently needed.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Caminero JA. Multidrug-resistant tuberculosis: epidemiology, risk factors and case finding [State of the art series. Drug-resistant tuberculosis. Edited by C-Y. Chiang. Number 4 in the series]. The International Journal of Tuberculosis and Lung Disease. 2010;14(4):382–90. - PubMed
-
- Caminero JA. Likelihood of generating MDR-TB and XDR-TB under adequate National Tuberculosis Control Programme implementation [Review article]. The International Journal of Tuberculosis and Lung Disease. 2008;12(8):869–77. - PubMed
-
- Van Rie A, Warren R, Richardson M, Gie RP, Enarson DA, Beyers N, et al. Classification of drug-resistant tuberculosis in an epidemic area. The Lancet. 2000;356(9223):22–5. - PubMed
-
- WHO. Policy Update: Xpert MTB/RIF assay for the diagnosis of pulmonary and extrapulmonary TB in adults and children. Geneva 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
