

Differences and similarities in the effects of ibrutinib and acalabrutinib on platelet functions
- PMID: 30819914
- PMCID: PMC6821604
- DOI: 10.3324/haematol.2018.207183
Differences and similarities in the effects of ibrutinib and acalabrutinib on platelet functions
Abstract
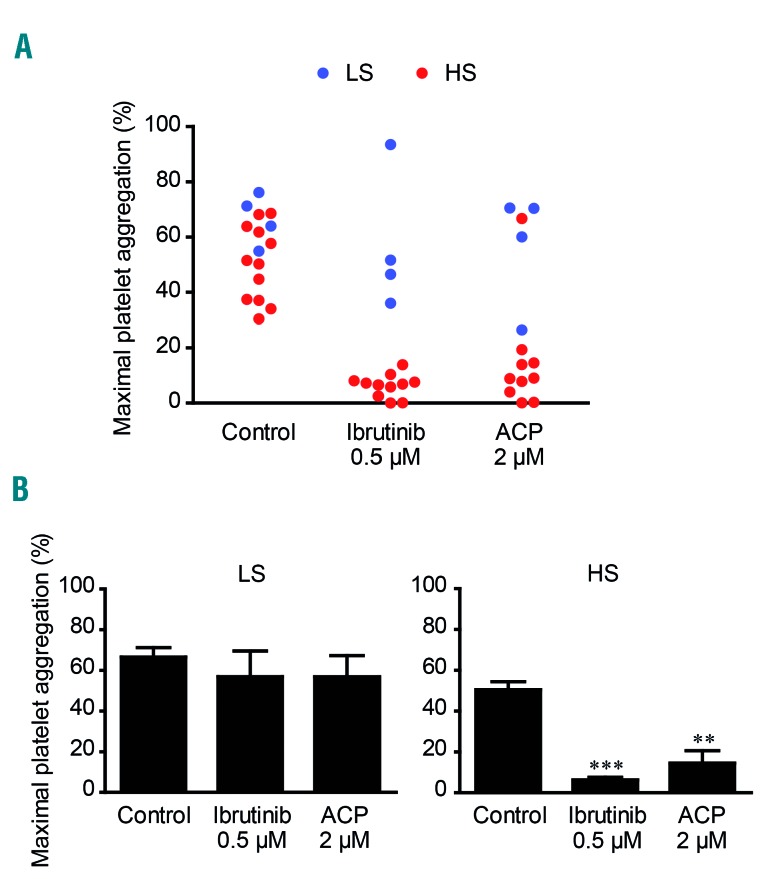
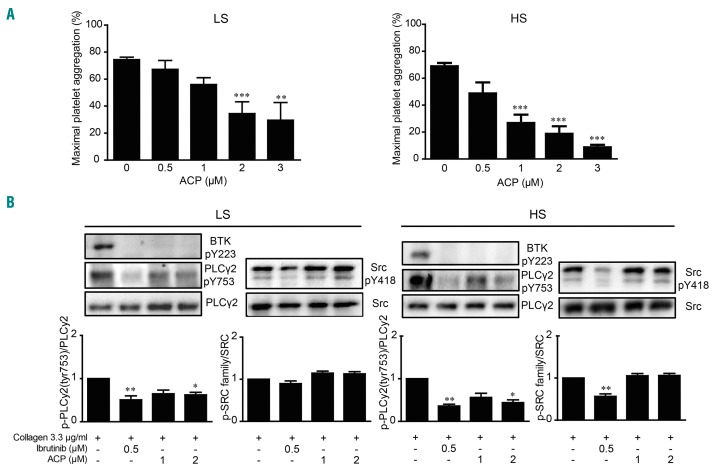
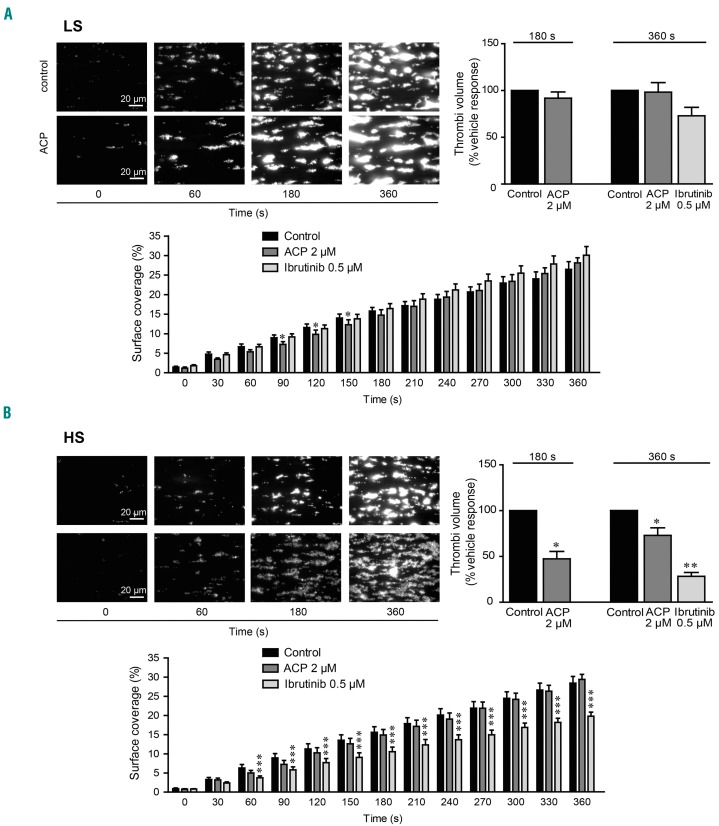
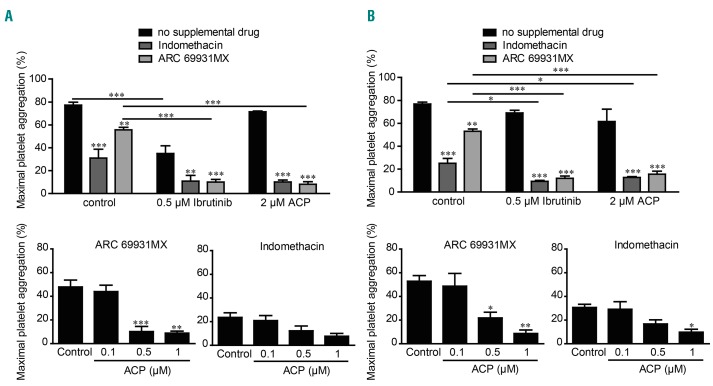
While efficient at treating B-cell malignancies, Bruton tyrosine kinase (BTK) inhibitors are consistently reported to increase the risk of bleeding. Analyzing platelet aggregation response to collagen in platelet-rich plasma allowed us to identify two groups in the healthy population characterized by low or high sensitivity to ibrutinib in vitro Inhibition of drug efflux pumps induced a shift from ibrutinib low-sensitive platelets to high-sensitive ones. At a clinically relevant dose, acalabrutinib, a second-generation BTK inhibitor, did not affect maximal collagen-induced platelet aggregation in the ibrutinib low-sensitive group but did inhibit aggregation in a small fraction of the ibrutinib high-sensitive group. Consistently, acalabrutinib delayed aggregation, particularly in the ibrutinib high-sensitive group. In chronic lymphocytic leukemia patients, acalabrutinib inhibited maximal platelet aggregation only in the ibrutinib high-sensitive group. Acalabrutinib inhibited collagen-induced tyrosine-753 phosphorylation of phospholipase Cγ2 in both groups, but, in contrast to ibrutinib, did not affect Src-family kinases. Acalabrutinib affected thrombus growth under flow only in the ibrutinib high-sensitive group and potentiated the effect of cyclooxygenase and P2Y12 receptor blockers in both groups. Since the better profile of acalabrutinib was observed mainly in the ibrutinib low-sensitive group, replacement therapy in patients may not systematically reduce the risk of bleeding.
Copyright© 2019 Ferrata Storti Foundation.
Figures

References
-
- Seiler T, Dreyling M. Bruton’s tyrosine kinase inhibitors in B-cell lymphoma: current experience and future perspectives. Expert Opin Investig Drugs. 2017;26(8):909–915. - PubMed
-
- Chakraborty R, Kapoor P, Ansell SM, Gertz MA. Ibrutinib for the treatment of Waldenström macroglobulinemia. Expert Rev Hematol. 2015;8(5):569–579. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
Miscellaneous
